28 Feb, 2025 | Admin | No Comments
France has just banned nicotine pouch sales. Where else in Europe are they restricted?
Several countries have taken steps to restrict nicotine pouches absent EU-wide regulation.
12 Feb, 2025 | Admin | No Comments
Old people in England are happier with their life now than before COVID. What’s changed?
Older adults in England reported better mental well-being after the pandemic, but also slightly elevated depression rates.
29 May, 2024 | Admin | No Comments
Considering (or currently taking) weight loss drugs? Here’s what you need to know
If you live in a larger body, sometimes it feels like you can’t win.
If you don’t lose weight, people will criticize you for being “lazy,” “unhealthy,” or “lacking willpower.”
But if you take medication to help you, you’ll be criticized for “cheating” or “taking the easy way out,” even if you’ve tried for decades to manage your weight through diet, exercise, and lifestyle changes (sometimes extreme ones).
In this article, we’ll be talking about a highly contentious group of medicines—GLP-1 receptor agonist drugs such as semaglutide (Ozempic, Wegovy, Rybelsus) or tirzepatide (Mounjaro, Zepbound).
And people have lots of opinions about them.
But the opinion that matters most? Yours.
At PN, we’re medication agnostic.
We’re not here to judge whether a person should or should not take medication for weight loss. Ultimately, that’s a choice left up to you, with the guidance of your primary care physician.
Either way, we’re here to support our clients and elevate their results.
Whether you take medication or not, a coach can help you optimize nutrition and satiety with the right foods, find exercises that work with your changing body, and help you navigate the emotional ups and downs that come when you attempt to tackle a big, meaningful, long-term goal.
However, we also understand that if you’re debating the pros and cons of beginning (or continuing) medication, you might have mixed feelings.
If you’re not sure if these new medicines are right for you, we have your back. In the following article, we’ll give you the honest, science-backed information you need to make a confident decision.
You’ll learn…
- Why it’s so hard to lose (and keep off) fat
- Why taking medication isn’t “cheating,” nor is it the “easy way out”
- How GLP-1 drugs work, and the health benefits they can have (aside from weight loss)
- How to determine if you’re at a “healthy weight” (it’s not just about BMI)
- What actions you can take to minimize side effects and maximize long-term health, if you do decide to take these medications
Let’s begin.
First, why is it so hard to lose fat?
Fat loss is hard. Period.
But for some people, it’s harder still—because of environmental, genetic, physiological, social, cultural, and/or behavioral factors that work against them.
Here are a few of the contributing factors that can make fat loss so challenging.
We live in an environment that encourages a caloric surplus.
Imagine life 150 years ago, before cars and public transit were invented. To get from point A to point B, you had to walk, pedal a bicycle, or ride a horse.
Food was often in short supply, too. You had to expend calories to get it, and meals would just satisfy you (but not leave you “full”).
Today, however…
“We live in an obesogenic environment that’s filled with cheap, highly-palatable, energy-dense foods [that make overeating calories easy, often unconsciously],” says Karl Nadolsky, MD, an endocrinologist and weight loss specialist at Holland Hospital and co-host of the Docs Who Lift podcast.
“We also have countless conveniences that reduce our physical activity.”
Of course, even in such an environment, we have people in lean bodies, just as we have people who struggle to stop the scale from continuously creeping up.
Why?
Genetically, some people are more predisposed to obesity.
Some genes can lead to severe obesity at a very early age. However, those are pretty rare.
Much more common is polygenic obesity—when two or more genes work together to predispose you to weight gain, especially when you’re exposed to the obesogenic environment mentioned earlier.
People who inherit one or more of these so-called obesity genes tend to have particularly persistent “I’m hungry” and “I’m not full yet” signals, says Dr. Nadolsky.
Obesity genes also seem to cause some people to experience what’s colloquially known as “food noise.”
They feel obsessed with food, continually thinking, “What am I going to eat next? When is my next meal? Can I eat now?”
Physiologically, bodies tend to resist fat loss.
If you gain a lot of fat, the hormones in your gut, fat cells, and brain can change how you experience hunger and fullness.
“It’s like a thermostat in a house, but now it’s broken,” says Dr. Nadolsky. “So when people cut calories and weight goes down, these physiologic factors work against them.”
After losing weight, your gut may continually send out the “I’m hungry” signal, even if you’ve recently eaten, and even if you have more than enough body fat to serve as a calorie reserve. It also might take more food for you to feel full than, say, someone else who’s never been at a higher weight.
Being in a larger body often means being the recipient of fat stigma and discriminatory treatment.
Until you’ve lived in a larger body, it’s hard to believe how different the world might treat you.
Our clients have told us stories about being bullied at the gym, openly judged or lectured at the grocery store, and otherwise being subjected to innumerable comments and assumptions about their body shape, health, and even worth.
Even in medical settings, people with obesity are more likely to receive poor treatment.1, 2 Healthcare providers may overlook or downplay symptoms, attributing health concerns solely to weight. This can lead to delayed- or missed diagnoses or just plain old inadequate care.
All of this combined can add up to an incredibly pervasive and ongoing source of stress.
This stress—in addition to being socially isolating and psychologically damaging—can further contribute to increased appetite and pleasure from high-calorie foods, decreased activity, and poorer sleep quality.3
Which is why…
Taking medication isn’t an “easy way out.”
In 2013, the American Medical Association categorized obesity as a disease.
And yet, many people still don’t treat it as such, and rather consider obesity as a willpower problem, and the consequence of simply eating too much and moving too little. (The remedy: “Just try harder.”)
In reality, people with obesity have as much willpower as anyone else.
However, for them, fat loss is harder—for all the reasons mentioned above, and more.
So, just like chemotherapy or insulin isn’t “the easy way out” of cancer or type 1 diabetes, medication isn’t “the easy way out” of obesity.
Rather, medication is a tool, ideally used alongside healthy lifestyle behaviors, that can help offset some of the genetic and physiological variances that people with obesity may have, and have little individual control over otherwise.
What you need to know about GLP-1 drugs
In 2017, semaglutide (a synthentic GLP-1 agonist) was approved in the US as an antidiabetic and anti-obesity medication.
With the emergence of this class of drugs, science offered people with obesity a relatively safe and accessible way to lose weight long-term, so long as they continued the medication.
How Ozempic and other obesity medicines work
Current weight loss medications work primarily by mimicking the function of glucagon-like peptide 1 (GLP-1), a hormone that performs several functions:
- In the pancreas, it triggers insulin secretion, which helps regulate blood sugar (and also helps you feel full).
- In the gut, it slows gastric emptying, affecting your sensation of fullness.
- In the brain, it reduces cravings (the desire for specific foods) and food noise (intrusive thoughts about food).
In people with obesity, the body quickly breaks down endogenous (natural) GLP-1, making it less effective. As a result, it takes longer to feel full, meals offer less staying power, and food noise becomes a near-constant companion, says Dr. Nadolsky.
Semaglutide and similar medicines flood the body with synthetically made GLP-1 that lasts much longer than the GLP-1 the body produces. This long-lasting effect helps increase feelings of fullness, reduce between-meal hunger, and muffle cravings and food noise.
Interestingly, by calming down the brain’s reward center (the part of the brain that drives cravings and even addictions), these medicines may also help people reduce addictive behaviors like compulsive drinking and gambling, says Dr. Nadolsky.
Note: Newer weight loss medicines, for example tirzepatide, mimic not only GLP-1, but also another hormone called gastric inhibitory polypeptide (GIP). Like GLP-1, GIP also stimulates post-meal insulin secretion and reduces appetite, partly by decreasing gastrointestinal activity. Other drugs soon to come on the market, like retatrutide, mimic a third hormone, glucagon.
How effective are GLP-1 drugs?
Researchers measure a weight loss medicine’s success based on the percentage of people who reach key weight loss milestones of 5, 10, 15, or 20 percent of their weight.
These medicines are still evolving, but so far, they have shown to be quite effective:
About 86 percent of people who take GLP-1 drugs like Ozempic, Rybelsus, and Wegovy lose at least five percent of their body weight, with about a third of them losing more than 20 percent of their body weight.4, 5
And newer generation versions of these medications—such as tirzepatide, and the not-yet-FDA-approved retatrutide—are only getting better, with up to 57 percent of people losing more than 20 percent of their body weight.6, 7
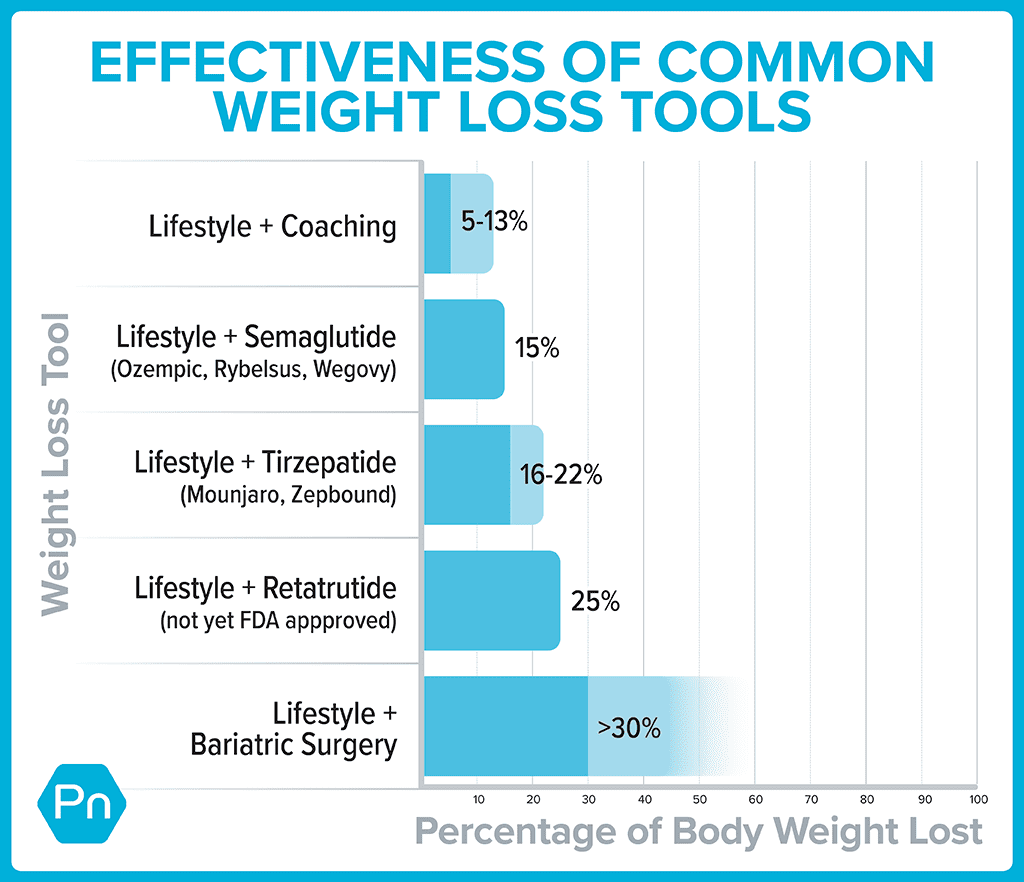
How do weight loss medications compare to lifestyle interventions?
In the past, weight loss interventions have focused on lifestyle modifications like calorie or macronutrient manipulation, exercise, and sometimes counseling.
Rather than pitting lifestyle changes against weight loss medicines or surgery, it’s more helpful to think of them all as compatible players.
With lifestyle modifications and coaching, the average person can expect to lose about five to 13 percent of their body weight.
When you add FDA-approved versions of GLP-1 and other weight-loss drugs to lifestyle and coaching, average weight loss jumps up another ten percent or more. 8, 9, 10, 11
Fat loss often comes with powerful health benefits
For years, the medical community has told folks that losing 5 to 10 percent of their body weight was good enough.
Partly, this message was designed to right-set people’s expectations, as few lose much more than that (and keep it off) with lifestyle changes alone.
In addition, this modest weight loss also leads to measurable health improvements. Lose 5 to 10 percent of your total weight, and you’ll start to see blood sugar, cholesterol, and pressure drop.12
However, losing 15 to 20 percent of your weight, as people tend to do when they combine lifestyle changes with second-generation GLP-1s, and you do much more than improve your health. You can go into remission for several health problems, including:
- High blood pressure
- Diabetes
- Fatty liver disease
- Sleep apnea
That means, by taking a GLP-1 medicine, you might be able eventually to stop taking several other drugs, says Dr. Nadolsky.
Experts suspect GLP-1s may improve health even when no weight loss occurs.
“The medicines seem to offer additive benefits beyond just weight reduction,” says Dr. Nadolsky.
Research indicates that GLP-1s may reduce the risk of major cardiovascular events (heart attacks and strokes) in people with diabetes or heart disease.13, 14, 15 In people with diabetes, they seem to improve kidney function, too.16
The theory is that organs throughout the body have GLP-1 receptors on their cells. When the GLP-1s attach to these receptors in the kidneys and heart, they seem to protect these organs from damage.
For this reason, in 2023, the American Heart Association listed GLP-1 receptor agonists as one of the year’s top advances in cardiovascular disease.
What even is a “healthy body weight”?
Many people say, “I just want to be at a healthy weight.”
But what does that even mean?
At PN, we believe your healthiest body composition / weight is one that:
- Has relatively more lean mass (from muscle and healthy, dense bones), and relatively less body fat
- Emerges from doing foundational, sustainable health-promoting behaviors (like being active and eating well), rather than “crash diets” or other extreme measures
- Is relatively easy to maintain with a handful of consistent lifestyle choices, without undue sacrifices to overall well-being (or what we call Deep Health)
- Allows you to do the activities you want and enjoy, with as few limitations as possible
- Keeps your health markers (like blood pressure, cholesterol, and blood sugar) in safe and healthy ranges as much as is reasonably possible
- Feels good to you
This is not a specific size, shape, look, body fat percentage, or category on a BMI chart; A “healthy” body composition and/or weight will vary from person to person.
… Which can be both freeing and frustrating to hear.
Without a specific number to aim for, it’s harder to know if you’ve “arrived” at your healthiest weight or body composition.
However, we like this way of qualifying what a healthy weight is because it takes the pressure off a number on the scale, and puts the focus on behaviors you have more control over, and more importantly, how your life feels.
7 strategies to make weight loss medicines more effective—and improve long-term health
Here’s what we believe:
Weight loss medicines don’t render lifestyle changes obsolete; they make them more critical.
When GLP-1 medicines muffle food noise and hunger, many find it easier to prioritize lean protein, fruits and veggies, whole grains, and other minimally processed foods. Similarly, as the scale goes down, people often feel better, so they’re more likely to embrace weight lifting and other forms of exercise.
Indeed, according to a 2024 consumer trends survey, 41 percent of GLP-1 medicine users reported that their exercise frequency increased since going on the medication. The majority of them also reported an improvement in diet quality, choosing to eat more protein, as well as fruits and vegetables.17
This is great news, because it further reinforces the idea that medication isn’t simply “the easy way out.”
(Of course, sometimes drugs are used as “the easy way out”; After going on medication, people can continue to eat poor quality food—just less of it. This increases the risk of losing critical muscle and bone, and losing less—or even no—body fat.)
When used correctly, weight loss medication is a tool that, as mentioned above, can make healthy lifestyle changes easier to accomplish, making both the drugs and the lifestyle changes more effective, and enhancing both short- and long-term success.
If you do decide to take weight loss drugs, use these strategies to get the most out of them—and preserve your long-term health.
Strategy #1: Find ways to eat nutritiously despite side effects.
The slowed stomach emptying caused by GLP-1 drugs can trigger nausea and constipation.
Fortunately, for most people, these GI woes tend to resolve within several weeks.
However, if you’re experiencing a lot of nausea, you’re not likely going to welcome salads into your life with open arms. (Think of how you feel when you have the stomach flu. A bowl of roughage doesn’t seem like it’ll “go down easy.”)
So, try to find more palatable ways to consume nutritious foods. (For example, fruits and vegetables in the form of a smoothie or pureed soup might be easier.)
Dr. Nadolsky also suggests people avoid the following common offenders:
- Big portions of any kind
- Greasy, fatty foods
- Highly processed foods
- Any strong food smells that trigger your gag reflex
- Sugar alcohols (like xylitol, erythritol, maltitol, and sorbitol, often found in diet sodas, chewing gum, and low-sugar protein bars), which can trigger diarrhea in some
Strategy #2: Prioritize strength training.
When people take GLP-1 weight loss medicines, about 30 to 40 percent of the weight they lose can come from lean mass.18, 19, 20
Put another way: For every 10 pounds someone loses, about six to seven come from fat and three to four from muscle, bone, and other non-fat tissues.
However, there’s two important caveats to this statistic:
1. People with severe obesity generally have more muscle and bone mass than others. (Carrying around an extra 100+ pounds of body weight means muscles have to adapt by getting bigger and stronger.)
2. Muscle and bone loss aren’t inevitable. (As Dr. Nadolsky puts it, “Muscle loss isn’t a reason to avoid treating obesity [with medication]. It’s a reason to do more exercise.”)
To preserve muscle and bone mass, aim for at least two full-body resistance training sessions a week.
In addition, move around as much as you can. Walking and other forms of physical activity are vital for keeping metabolism healthy—and can help to move food through the gut to ease digestion.21, 22
(Need inspiration for strength training? Check out our free exercise video library.)
Strategy #3: Lean into lean protein.
In addition to strength training, adequate protein consumption is vital for helping to protect muscle mass.
You can use our free macros calculator to determine the right amount of protein for you. (Spoiler: Most people will need 1 to 2 palm-sized protein portions per meal, or about 0.5 to 1 gram of protein per pound of body weight per day.)
Strategy #4: Fill your plate with fruit and veggies.
Besides being good for your overall health, whole, fresh, and frozen produce fuels you with critical nutrients that can help drive down levels of inflammation.
In addition to raising your risk for disease, chronic inflammation can block protein synthesis, making it harder to maintain muscle mass.
(Didn’t know managing inflammation matters when it comes to preserving muscle? Find out more muscle-supporting strategies here: How to build muscle strength, size, and power)
Strategy #5: Choose high-fiber carbs over low-fiber carbs.
Beans, lentils, whole grains, and starchy tubers like potatoes and sweet potatoes do a better job of helping you feel full and managing blood sugar than lower-fiber, more highly processed options.
(Read more about the drawbacks—and occasional benefits—of processed foods here: Minimally processed vs. highly processed foods)
Strategy #6: Choose healthy fats.
Healthy fats can help you feel full between meals and protect your overall health.
Gravitate toward fats from whole foods like avocado, seeds, nuts, and olive oil, as well as fatty fish (which is a protein too!)—using them to replace less healthy fats from highly-processed foods (like chips or donuts).
(Not sure which fats are healthy? Use our 3-step guide for choosing the best foods for your body)
Strategy #7: Consider coaching.
It may go without saying, but the above suggestions are just the start.
(There’s also: quality sleep, social support, stress management, and more.)
While many people choose to tackle these strategies on their own, many others find that the support, guidance, and creative problem-solving that a good coach can provide makes the whole process a lot easier—not to mention more enjoyable and more likely to stick.
And that’s the real gift of coaching: A coach doesn’t just help you figure out what to eat and how to move; They help you remove barriers, build skills, and create systems and routines so that habits become so natural and automatic that it’s hard to imagine not doing them.
Then, if you do want to stop taking medication, your ingrained lifestyle habits (that coaching reinforced, and medication perhaps made easier to adopt) will make it more likely that you maintain your results.
jQuery(document).ready(function(){
jQuery(“#references_link”).click(function(){
jQuery(“#references_holder”).show();
jQuery(“#references_link”).parent().hide();
});
});
References
Click here to view the information sources referenced in this article.
1. Phelan, S. M., D. J. Burgess, M. W. Yeazel, W. L. Hellerstedt, J. M. Griffin, and M. van Ryn. 2015. “Impact of Weight Bias and Stigma on Quality of Care and Outcomes for Patients with Obesity.” Obesity Reviews: An Official Journal of the International Association for the Study of Obesity 16 (4): 319–26.
2. Tomiyama, A. Janet, Deborah Carr, Ellen M. Granberg, Brenda Major, Eric Robinson, Angelina R. Sutin, and Alexandra Brewis. 2018. “How and Why Weight Stigma Drives the Obesity ‘Epidemic’ and Harms Health.” BMC Medicine 16 (1).
3. Tomiyama, A. Janet. 2019. “Stress and Obesity.” Annual Review of Psychology 70 (1): 703–18.
4. Wilding JPH, Batterham RL, Calanna S, Davies M, Van Gaal LF, Lingvay I, et al. Once-Weekly Semaglutide in Adults with Overweight or Obesity. N Engl J Med. 2021 Mar 18;384(11):989–1002
5. Garvey WT, Batterham RL, Bhatta M, Buscemi S, Christensen LN, Frias JP, et al. Two-year effects of semaglutide in adults with overweight or obesity: the STEP 5 trial. Nat Med. 2022 Oct;28(10):2083–91.
6. le Roux CW, Zhang S, Aronne LJ, Kushner RF, Chao AM, Machineni S, et al. Tirzepatide for the treatment of obesity: Rationale and design of the SURMOUNT clinical development program. Obesity. 2023 Jan;31(1):96–110.
7. Jastreboff AM, Aronne LJ, Ahmad NN, Wharton S, Connery L, Alves B, et al. Tirzepatide Once Weekly for the Treatment of Obesity. N Engl J Med. 2022 Jul 21;387(3):205–16..
8. Leung, Alice W. Y., Ruth S. M. Chan, Mandy M. M. Sea, and Jean Woo. 2017. “An Overview of Factors Associated with Adherence to Lifestyle Modification Programs for Weight Management in Adults.” International Journal of Environmental Research and Public Health 14 (8).
9. Jastreboff, Ania M., Louis J. Aronne, Nadia N. Ahmad, Sean Wharton, Lisa Connery, Breno Alves, Arihiro Kiyosue, et al. 2022. “Tirzepatide Once Weekly for the Treatment of Obesity.” The New England Journal of Medicine 387 (3): 205–16.
10. Jastreboff, Ania M., Lee M. Kaplan, Juan P. Frías, Qiwei Wu, Yu Du, Sirel Gurbuz, Tamer Coskun, Axel Haupt, Zvonko Milicevic, and Mark L. Hartman. 2023. “Triple–Hormone-Receptor Agonist Retatrutide for Obesity — A Phase 2 Trial.” The New England Journal of Medicine 389 (6): 514–26.
11. Maciejewski, Matthew L., David E. Arterburn, Lynn Van Scoyoc, Valerie A. Smith, William S. Yancy Jr, Hollis J. Weidenbacher, Edward H. Livingston, and Maren K. Olsen. 2016. “Bariatric Surgery and Long-Term Durability of Weight Loss.” JAMA Surgery 151 (11): 1046–55.
12. Ryan DH, Yockey SR. Weight Loss and Improvement in Comorbidity: Differences at 5%, 10%, 15%, and Over. Curr Obes Rep. 2017 Jun;6(2):187–94.
13. Marx N, Husain M, Lehrke M, Verma S, Sattar N. GLP-1 Receptor Agonists for the Reduction of Atherosclerotic Cardiovascular Risk in Patients With Type 2 Diabetes. Circulation. 2022 Dec 13;146(24):1882–94.
14. Lincoff AM, Brown-Frandsen K, Colhoun HM, Deanfield J, Emerson SS, Esbjerg S, et al. Semaglutide and Cardiovascular Outcomes in Obesity without Diabetes. N Engl J Med. 2023 Dec 14;389(24):2221–32.
15. Kosiborod MN, Abildstrøm SZ, Borlaug BA, Butler J, Rasmussen S, Davies M, et al. Semaglutide in Patients with Heart Failure with Preserved Ejection Fraction and Obesity. N Engl J Med. 2023 Sep 21;389(12):1069–84.
16. Karakasis P, Patoulias D, Fragakis N, Klisic A, Rizzo M. Effect of tirzepatide on albuminuria levels and renal function in patients with type 2 diabetes mellitus: A systematic review and multilevel meta-analysis. Diabetes Obes Metab [Internet]. 2023 Dec 20
17. N.d. Accessed May 21, 2024. https://newconsumer.com/wp-content/uploads/2024/03/Consumer-Trends-2024-Food-Wellness-Special.pdf
18. Ida S, Kaneko R, Imataka K, Okubo K, Shirakura Y, Azuma K, et al. Effects of Antidiabetic Drugs on Muscle Mass in Type 2 Diabetes Mellitus. Curr Diabetes Rev. 2021;17(3):293–303.
19. Wilding JPH, Batterham RL, Calanna S, Van Gaal LF, McGowan BM, Rosenstock J, et al. Impact of Semaglutide on Body Composition in Adults With Overweight or Obesity: Exploratory Analysis of the STEP 1 Study. J Endocr Soc. 2021 May 3;5(Supplement_1):A16–7.
20. Wilding JPH, Batterham RL, Calanna S, Davies M, Van Gaal LF, Lingvay I, et al. Once-Weekly Semaglutide in Adults with Overweight or Obesity. N Engl J Med. 2021 Mar 18;384(11):989–1002.
21. Gorgojo-Martínez JJ, Mezquita-Raya P, Carretero-Gómez J, Castro A, Cebrián-Cuenca A, de Torres-Sánchez A, et al. Clinical Recommendations to Manage Gastrointestinal Adverse Events in Patients Treated with Glp-1 Receptor Agonists: A Multidisciplinary Expert Consensus. J Clin Med Res [Internet]. 2022 Dec 24;12(1).
22. Tantawy SA, Kamel DM, Abdelbasset WK, Elgohary HM. Effects of a proposed physical activity and diet control to manage constipation in middle-aged obese women. Diabetes Metab Syndr Obes. 2017 Dec 14;10:513–9.
Want help becoming the healthiest, fittest, strongest version of you?
Most people know that regular movement, eating well, sleep, and stress management are important for looking and feeling better. Yet they need help applying that knowledge in the context of their busy, sometimes stressful lives.
Over the past the past two decades, we’ve used the Precision Nutrition Coaching method to help over 150,000 clients lose fat, get stronger, and improve their physical and mental health… for the long-term… no matter what challenges they’re dealing with.
It’s also why we work with health, fitness, and wellness professionals (through our Level 1 and Level 2 Certification programs) to teach them how to coach their own clients through the same challenges.
<!–
Interested in Precision Nutrition Coaching? Join the presale list now. You’ll get a free gift today, save up to [pnc_discount], and have the chance to secure a spot 1 week early.
We’ll be opening up spots in our next Precision Nutrition Coaching on [launch_date program=”pnc” type=”general” dateformat=”l, F jS, Y”].
If you’re interested in coaching and want to find out more, join the presale list below. Being on the list gives you three special advantages.
- You’ll pay less than everyone else. Join the presale list and you’ll save up to [pnc_discount] off the general public price.
- You’re more likely to get a spot. To give clients the personal care and attention they deserve, we only open up the program twice a year. By joining the presale list you’ll get the opportunity to register a week before everyone else, increasing your chances of getting in.
- You’ll get a free gift—plus an inside look at the program. When you join the presale list today, we’ll send you a free 35-page ebook: Your Best Nutrition Starts Here—a complete guide to building a health plan for your body, goals, and lifestyle (no calorie-counting or restrictive dieting required). Plus, you’ll get our new Enrollment Packet, giving you an inside look at the PN Coaching program, complete with stories from past clients who’ve overcome huge obstacles and achieved the transformation of their dreams, and more.
If you’re ready to change your body, and your life, with help from the world’s best coaches, this is your chance.
[Note: If your health and fitness are already sorted out, but you’re interested in helping others, check out our Precision Nutrition Level 1 Certification program].
–>
The post Considering (or currently taking) weight loss drugs? Here’s what you need to know appeared first on Precision Nutrition.
8 Apr, 2024 | Admin | No Comments
Ozempic for weight loss: What coaches (and clients) need to know about GLP-1 drugs
Angela Fitch’s family history of obesity caught up to her at age 40, when she was pregnant with her first child.
As a physician and obesity medicine specialist, Dr. Fitch knew the lifestyle levers to pull—and she had the financial means to yank them hard.
After giving birth, she lifted weights with a trainer twice a week. She sweated through one Peloton workout after another and tracked her food intake on MyFitnessPal.
Nevertheless, for the next decade, Dr. Fitch lost (and regained) the same five to ten pounds. Her blood pressure crept upward. Then came a sleep apnea diagnosis.
As her 50th birthday neared, Dr. Fitch decided to take the advice she gave her patients. She went on medication. (And, she lost 30 pounds.)
In the years since, Dr. Fitch has occasionally stopped her meds. For a few months, she maintains her results.
Eventually, however, the scale climbs back. For now, she’s decided that she’ll be on medication long-term.
If you’re a coach, how does this story land with you?
Does it…
… Make you feel disappointed? Does this seem like a story of someone “giving up” or “not trying hard enough”?
… Inspire you with a sense of awe? That modern medicine has figured out how to treat yet another chronic disease?
… Bring up questions? Like wondering about the effects of being on medication—potentially long-term? (Or if weight loss is even that relevant—so long as a person is eating healthy and exercising regularly?)
Dr. Fitch is now president of the Obesity Medicine Association and chief medical officer of Known Well, a primary care and obesity medicine practice in Needham, Massachusetts. Regardless of how you feel about her story, it illustrates what can initially seem like an inconvenient truth for those of us in the health coaching industry:
Behavior change on its own isn’t always enough.
For many people with obesity, semaglutide (Ozempic, Wegovy, Rebelsus), tirzepatide (Mounjaro, Zepbound), and other glucagon-like peptide-1 receptor agonists (GLP-1 RAs) serve as valuable tools that make significant and lasting weight loss possible.
But for health coaches, these drugs can seem like an existential threat.
You might wonder:
‘Who needs a nutrition coach or a personal trainer when people can get faster, easier, and more dramatic results with drugs?’
However…
People need health coaches now more than ever.
In this story, we’ll explain why—and show you how to turn “the golden age of obesity medicine” into a massive career opportunity.
With fat loss, there’s no such thing as an “easy way out.”
To manage diabetes or treat cancer, most people consider it normal and natural to combine lifestyle behaviors with prescription medicine.
No one would tell someone with cancer, “You’re on chemo? Way to take the easy way out!”
However, that’s what many people with obesity hear when they mention medication or surgery.
For decades, much of society hasn’t viewed obesity as the disease that it is.
Instead, people have seen it as a willpower problem.
The remedy: “Just try harder.”
However, rather than motivating people to succeed, this “remedy” often encourages them to give up. (More importantly, the willpower theory isn’t based on science.)
In reality, people with obesity likely have as much willpower as anyone else.
However, for them, fat loss is harder—because of genetics and physiology, along with social, cultural, behavioral, and/or environmental factors that work against them.
Why is it so difficult to lose fat?
Imagine life 150 years ago, before the invention of the automobile. To get from point A to point B, you had to walk, pedal a bicycle, or ride a horse.
Food was often in short supply, too. You had to expend calories to get it, and meals would just satisfy you (but not leave you feeling “full”).
Today, however…
“We live in an obesogenic environment that’s filled with cheap, highly-palatable, energy-dense foods [that make overeating calories easy, often unconsciously], and countless conveniences that reduce our physical activity,”
says Karl Nadolsky, MD, an endocrinologist and weight loss specialist at Holland Hospital and co-host of the Docs Who Lift podcast.
You might wonder: Why do some people gain fat in an obesity-promoting environment while others don’t?
The answer comes down to, in large part, genetics and physiology.
(Obesity is complex and multifactorial. As we noted above, there are other influential factors, but your genes and physiology are mostly out of your control, and so medication might be the best tool to modify their impact.)
Genetically, some people are more predisposed to obesity.
Some genes can lead to severe obesity at a very early age. However, those are pretty rare.
Much more common is polygenic obesity—when two or more genes work together to predispose you to weight gain, especially when you’re exposed to the obesogenic environment mentioned earlier.
People who inherit one or more of these so-called obesity genes tend to have particularly persistent “I’m hungry” and “I’m not full yet” signals, says Dr. Nadolsky.
Obesity genes also seem to cause some people to experience what’s colloquially known as “food noise.”
They feel obsessed with food, continually thinking, “What am I going to eat next? When is my next meal? Can I eat now?”
Physiologically, bodies tend to resist fat loss.
If you gain a lot of fat, the hormones in your gut, fat cells, and brain can change how you experience hunger and fullness.
“It’s like a thermostat in a house, but now it’s broken,” says Dr. Nadolsky. “So when people cut calories and weight goes down, these physiologic factors work against them.”
After losing weight, your gut may continually send out the “I’m hungry” signal, even if you’ve recently eaten, and even if you have more than enough body fat to serve as a calorie reserve. It also might take more food for you to feel full than, say, someone else who’s never been at a higher weight.
Enter: GLP-1 drugs
In 2017, semaglutide—a synthetic analog of the metabolic hormone glucagon-like peptide 1—was approved in the US as an antidiabetic and anti-obesity medication.
With the emergence of this class of drugs, science offered people with obesity a relatively safe and accessible way to lose weight long-term, so long as they continued the medication.
How Ozempic and other obesity medicines work
Current weight loss medications work primarily by mimicking the function of glucagon-like peptide 1 (GLP-1), which is a hormone that performs several functions:
- In the pancreas, it triggers insulin secretion, which helps regulate blood sugar.
- In the gut, it slows gastric emptying, affecting your sensation of fullness.
- In the brain, it reduces cravings (the desire for specific foods) and food noise (intrusive thoughts about food).
In people with obesity, the body quickly breaks down endogenous (natural) GLP-1, making it less effective. As a result, it takes longer to feel full, meals offer less staying power, and food noise becomes a near-constant companion, says Dr. Nadolsky.
Semaglutide (Ozempic, Wegovy, Rybelsus) and medicines like it flood the body with synthetically made GLP-1 that lasts much longer than the GLP-1 the body produces. This long-lasting effect helps increase feelings of fullness, reduce between-meal hunger, and muffle cravings and food noise.
Interestingly, by calming down the brain’s reward center, these medicines may also help people reduce addictive behaviors like problem drinking and compulsive gambling, says Dr. Nadolsky.
The lesser-known history of weight loss medicine
To understand the power of semaglutide (Ozempic, Wegovy, Rybelsus) and other GLP-1 medicines, it’s helpful to know a little about the drugs that predated it.
Decades before the age of Ozempic, physicians realized that several drugs originally developed to treat other conditions also seemed to help people lose weight.
These included:
- Qsymia, which pairs phentermine (an older weight loss medicine) with the epilepsy medicine topiramate
- Contrave, which combines the antidepressant bupropion (Wellbutrin) with naltrexone, used to treat addictions
- Metformin, a diabetes medicine
However, weight loss from these older medicines was modest, helping people to lose (and keep off) around 5 to 10 percent of their body weight.1 2 3
Around 2010, liraglutide (Victoza, Saxenda) was approved by the FDA to treat diabetes. Like Ozempic and other newer weight loss medicines, liraglutide mimics glucagon-like peptide-1 (GLP-1), but it’s less effective than the newer medicines.
Why does Ozempic get all the credit?
Ozempic has become the Kleenex of weight loss medicines—a name brand people toss around as if it’s generic.
This fame is at least partly earned: Dr. Fitch says that semaglutide (Ozempic, Rybelsus, Wegovy) also works more effectively than liraglutide, its GLP-1 predecessor.
“Semaglutide is 94 percent similar to our own GLP-1,” she says, “They’ve been able to make it closer and closer to the GLP-1 our bodies make.”
It also lasts longer than liraglutide, and more of it reaches the brain.
However, newer meds outperform Ozempic. (See the table in the section below.)
And there are other medicines—available orally rather than via injection—coming. These pills will be easier to mass produce, which will drive down costs and make GLP-1 medicines even more accessible to more people.
So, although Ozempic is the current reigning brand of the weight loss drug world, it may be ousted in time.
The growing effectiveness of weight loss drugs (especially in combination with lifestyle modifications)
Researchers measure a weight-loss medicine’s success based on the percentage of people who reach key weight loss milestones.
For example, most people start to see health benefits after losing five percent of their weight—and remission from disease after losing around 20 percent.
As the chart below shows, weight loss medicines have become increasingly effective at helping people to reach both milestones.
| Medicine | % of people who lose 5% of their weight | % of people who lose >20% of their weight |
|---|---|---|
| First-generation weight loss medicines (Qsymia, Contrave, Metformin) 4 5 6 | 53-80% | 10-20% |
| Semaglutide (Ozempic, Rybelsus, Wegovy) 7 8 | 86% | 32% |
| Tirzepatide (Mounjaro, Zepbound) 9 10 | 85-91% | 50-57% |
| Retatrutide (not yet FDA approved) 11 12 | 92-100% | 80-83% |
How do weight loss medications compare to traditional interventions?
In the past, weight loss interventions have focused on lifestyle modifications like calorie or macronutrient manipulation, exercise, and sometimes counseling.
Rather than pitting lifestyle changes against weight loss medicines or surgery, it’s more helpful to think of them all as tools.
As the graph below shows, the more weight loss tools someone uses—including coaching—the more significant the results.13 14 15 16
Fat loss often comes with powerful health benefits
For years, the medical community has told folks that losing 5 to 10 percent of their body weight was good enough.
Partly, this message was designed to right-set people’s expectations, as few lose much more than that (and keep it off) with lifestyle changes alone.
In addition, this modest weight loss also leads to measurable health improvements. Lose 5 to 10 percent of your total weight, and you’ll start to see blood sugar, cholesterol, and pressure drop.17
However, losing 15 to 20 percent of your weight, as people tend to do when they combine lifestyle changes with second-generation GLP-1s, and you do much more than improve your health. You can go into remission for several health problems, including:
- High blood pressure
- Diabetes
- Fatty liver disease
- Sleep apnea
That means, by taking a GLP-1 medicine, you might be able eventually to stop taking several other drugs, says Dr. Nadolsky.
Experts suspect GLP-1s may improve health even when no weight loss occurs.
“The medicines seem to offer additive benefits beyond just weight reduction,” says Dr. Nadolsky.
Research indicates that GLP-1s may reduce the risk of major cardiovascular events (heart attacks and strokes) in people with diabetes or heart disease.18 19 20 In people with diabetes, they seem to improve kidney function, too.21
The theory is that organs throughout the body have GLP-1 receptors on their cells. When the GLP-1s attach to these receptors in the kidneys and heart, they seem to protect these organs from damage.
For this reason, in 2023, the American Heart Association listed GLP-1 receptor agonists as one of the year’s top advances in cardiovascular disease.
Ozempic side effects
You’ve likely heard that slowed gastric emptying from GLP-1s can lead to nausea, constipation, and other GI woes.
That’s all true.
However, for most, these side effects are manageable, especially with the help of a few key strategies (which we’ll cover later).
For now, however, we’d like to hash out a particular downside you’ve likely heard about from the media—because it offers a huge opportunity for health coaches.
When people take GLP-1 weight loss medicines, about 30 to 40 percent of the weight they lose can come from lean mass.22 23 24
Put another way: For every 10 pounds someone loses, about six to seven come from fat and three to four from muscle, bone, and other non-fat tissues.
This statistic has been broadcast among many media outlets in recent weeks as a dire warning against taking Ozempic, Wegovy, or Zepbound.
Such stories often fail to mention two important caveats:
Caveat #1: People with severe obesity generally have more muscle and bone mass than others.
To understand why, imagine you were forced to wear a 100- or 200-pound body suit every day for a year. Everyday activities—getting in and out of chairs, walking to and from the mailbox, climbing steps into a building—would feel like a resistance workout.
That’s likely partly why bariatric surgery patients experience a nine-year extension on their life expectancy, despite 30 percent of their weight loss coming from lean mass. They have more muscle than average to begin with, and therefore can safely lose some.25 26
For people with severe obesity, the health boost from body fat loss offsets the health risk of muscle and bone loss, says Dr. Fitch.
That said, there’s a caveat to the caveat: People who are only 30 pounds or so overweight may not be starting out with muscle and bone mass to spare. Especially if they’re older, they may begin their weight loss journey already under-muscled, with relatively low bone density. In those people, another drop in lean mass and bone density can add up to big health problems.
However…
Caveat #2: Muscle and bone loss aren’t inevitable.
As Dr. Nadolsky puts it, “Muscle loss isn’t a reason to avoid treating obesity [with medication]. It’s a reason to do more exercise.”
This is where coaches can shine.
By showing clients how to adopt muscle-building behaviors like strength training, combined with adequate protein consumption, you can help people offset the worst of the side effects when taking these medicines.
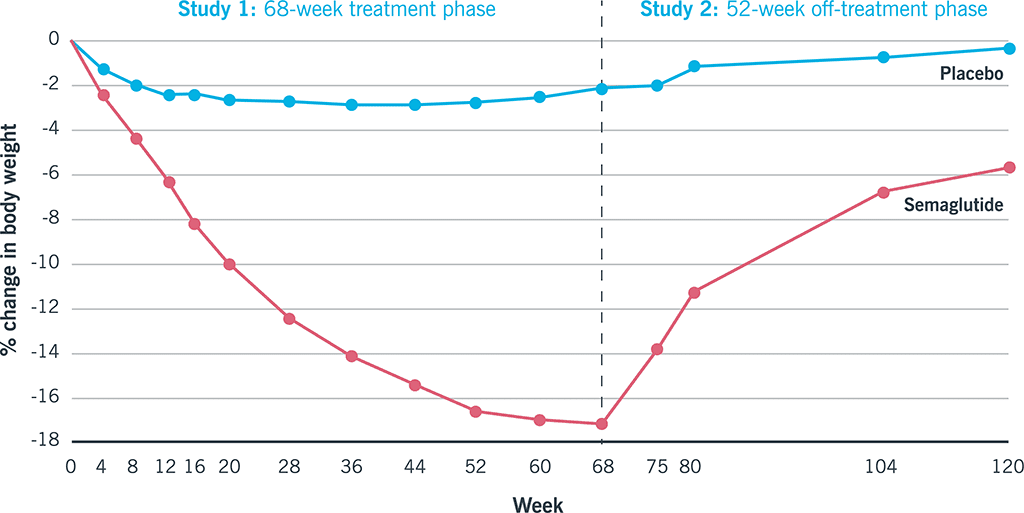
The yo-yo problem
GLP-1s are expensive, costing roughly $1000 USD a month. As a result, many insurers either refuse to cover them or limit their coverage to a year or two.
Once the money runs out, people tend to go off the meds—and the hunger and cravings return.
If they’ve done little to change their foundational eating habits, this puts them at a significant disadvantage. If they’re not eating slowly and mindfully and improving satiety with veggies and lean protein, the return of hunger and food noise can be overpowering.
That’s likely why, in one study, participants who stopped taking semaglutide regained, on average, two-thirds of the weight they’d lost.27
Again, here’s another opportunity for coaches…
Use weight loss medicine as a key that unlocks lifestyle changes.
Weight loss medicines don’t render behavior-based strategies obsolete; they make them more critical.
When GLP-1 medicines muffle food noise and hunger, your client will find it easier to prioritize protein, fruits and veggies, legumes, and other minimally processed whole foods. Similarly, as the scale goes down, clients feel better, so they’re more likely to embrace weight lifting and do other forms of exercise.
According to a 2024 consumer trends survey, 41 percent of GLP-1 medicine users reported that their exercise frequency increased since going on the medication. The majority of them also reported an improvement in diet quality, choosing to eat more protein, as well as fruits and vegetables.28
This is great news, because, as mentioned above, lifestyle changes are critical to preserving lean mass and preventing regain, should clients choose to discontinue medication.
When working with clients on GLP-1s, keep the following challenges in mind.
Coaching strategy #1: Find ways to eat nutritiously despite side effects.
The slowed stomach emptying caused by GLP-1 drugs can trigger nausea and constipation.
Fortunately, for most people, these GI woes tend to resolve within several weeks.
However, if you’re working with a client who’s experiencing a lot of nausea, they won’t likely welcome salads into their lives with open arms. (Think of how you feel when you have the stomach flu. A bowl of roughage doesn’t seem like it’ll “go down easy.”)
Instead, help clients find more palatable ways to consume nutritious foods. (For example, fruits and vegetables in the form of a smoothie or pureed soup might be easier.)
Dr. Nadolsky also suggests people avoid the following common offenders:
- Big portions of any kind
- Greasy, fatty foods
- Highly processed foods
- Any strong food smells that trigger a client’s gag reflex
- Sugar alcohols (like xylitol, erythritol, maltitol, and sorbitol, often found in diet sodas, chewing gum, and low-sugar protein bars), which can trigger diarrhea in some
Coaching strategy #2: Prioritize strength training.
To preserve muscle mass, aim for at least two full-body resistance training sessions a week.
In addition, move around as much as you can. Walking and other forms of physical activity are vital for keeping the weight off—and can help to move food through the gut to ease digestion.29 30
(Need inspiration for strength training? Check out our free exercise video library.)
Coaching strategy #3: Lean into lean protein.
In addition to strength training, protein is vital for helping to protect muscle mass.
You can use our free macros calculator to determine the right amount of protein for you or your client. (Spoiler: Most people will need 1 to 2 palm-sized protein portions per meal, or about 0.5 to 1 gram of protein per pound of bodyweight per day.)
Coaching strategy #4: Fill your plate with fruit and veggies.
Besides being good for your overall health, whole, fresh, and frozen produce fuels you with critical nutrients that can help drive down levels of inflammation.
In addition to raising your risk for disease, chronic inflammation can block protein synthesis, making it harder to maintain muscle mass.
(Didn’t know managing inflammation matters when it comes to preserving muscle? Find out more muscle-supporting strategies here: How to build muscle strength, size, and power)
Coaching strategy #5: Choose high-fiber carbs over low-fiber carbs.
Beans, lentils, whole grains, and starchy tubers like potatoes and sweet potatoes are more likely to help clients feel full and manage blood sugar than lower-fiber, more highly processed options.
(Read more about the drawbacks—and occasional benefits—of processed foods here: Minimally processed vs. highly processed foods.)
Coaching strategy #6: Choose healthy fats.
Healthy fats can help you feel full between meals and protect your overall health. Gravitate toward fats from whole foods like avocado, fatty fish (which is also a protein!), seeds, nuts, and olive oil—using them to replace less healthy fats from highly processed foods.
(Not sure which fats are healthy? Use our 3-step guide for choosing the best foods for your body.)
Coaching strategy #7: Build resilient habits.
It may go without saying, but the above suggestions are just the start.
(There’s also: quality sleep, social support, stress management, and more.)
Most importantly, clients need your help to make all of the above easier and more automatic.
And that’s the real gift of coaching: You’re not merely helping clients figure out what to eat and how to move; You’re showing them how to remove barriers and create systems and routines so their road to health is a little smoother.
That way, if they do need to stop taking medication, their ingrained lifestyle habits (that the medicine made easier for them to adopt) will make it more likely that they maintain their results.
jQuery(document).ready(function(){
jQuery(“#references_link”).click(function(){
jQuery(“#references_holder”).show();
jQuery(“#references_link”).parent().hide();
});
});
References
Click here to view the information sources referenced in this article.
- Hendricks EJ. Off-label drugs for weight management. Diabetes Metab Syndr Obes. 2017 Jun 10;10:223–34.
- Lonneman DJ Jr, Rey JA, McKee BD. Phentermine/Topiramate extended-release capsules (qsymia) for weight loss. P T. 2013 Aug;38(8):446–52.
- Sherman MM, Ungureanu S, Rey JA. Naltrexone/Bupropion ER (Contrave): Newly Approved Treatment Option for Chronic Weight Management in Obese Adults. P T. 2016 Mar;41(3):164–72.
- Apolzan JW, Venditti EM, Edelstein SL, Knowler WC, Dabelea D, Boyko EJ, et al. Long-Term Weight Loss With Metformin or Lifestyle Intervention in the Diabetes Prevention Program Outcomes Study. Ann Intern Med. 2019 May 21;170(10):682–90.
- Sherman MM, Ungureanu S, Rey JA. Naltrexone/Bupropion ER (Contrave): Newly Approved Treatment Option for Chronic Weight Management in Obese Adults. P T. 2016 Mar;41(3):164–72.
- Lonneman DJ Jr, Rey JA, McKee BD. Phentermine/Topiramate extended-release capsules (qsymia) for weight loss. P T. 2013 Aug;38(8):446–52.
- Wilding JPH, Batterham RL, Calanna S, Davies M, Van Gaal LF, Lingvay I, et al. Once-Weekly Semaglutide in Adults with Overweight or Obesity. N Engl J Med. 2021 Mar 18;384(11):989–1002.
- Garvey WT, Batterham RL, Bhatta M, Buscemi S, Christensen LN, Frias JP, et al. Two-year effects of semaglutide in adults with overweight or obesity: the STEP 5 trial. Nat Med. 2022 Oct;28(10):2083–91.
- le Roux CW, Zhang S, Aronne LJ, Kushner RF, Chao AM, Machineni S, et al. Tirzepatide for the treatment of obesity: Rationale and design of the SURMOUNT clinical development program. Obesity. 2023 Jan;31(1):96–110.
- Jastreboff AM, Aronne LJ, Ahmad NN, Wharton S, Connery L, Alves B, et al. Tirzepatide Once Weekly for the Treatment of Obesity. N Engl J Med. 2022 Jul 21;387(3):205–16.
- Jastreboff AM, Kaplan LM, Frías JP, Wu Q, Du Y, Gurbuz S, et al. Triple-Hormone-Receptor Agonist Retatrutide for Obesity – A Phase 2 Trial. N Engl J Med. 2023 Aug 10;389(6):514–26.
- Frias JP, Deenadayalan S, Erichsen L, Knop FK, Lingvay I, Macura S, et al. Efficacy and safety of co-administered once-weekly cagrilintide 2·4 mg with once-weekly semaglutide 2·4 mg in type 2 diabetes: a multicentre, randomised, double-blind, active-c,ontrolled, phase 2 trial. Lancet. 2023 Aug 26;402(10403):720–30.
- Leung, Alice W. Y., Ruth S. M. Chan, Mandy M. M. Sea, and Jean Woo. 2017. An Overview of Factors Associated with Adherence to Lifestyle Modification Programs for Weight Management in Adults. International Journal of Environmental Research and Public Health 14 (8).
- Maciejewski, Matthew L., David E. Arterburn, Lynn Van Scoyoc, Valerie A. Smith, William S. Yancy Jr, Hollis J. Weidenbacher, Edward H. Livingston, and Maren K. Olsen. 2016. Bariatric Surgery and Long-Term Durability of Weight Loss. JAMA Surgery 151 (11): 1046–55.
- Ryan DH, Yockey SR. Weight Loss and Improvement in Comorbidity: Differences at 5%, 10%, 15%, and Over. Curr Obes Rep. 2017 Jun;6(2):187–94.
- Marx N, Husain M, Lehrke M, Verma S, Sattar N. GLP-1 Receptor Agonists for the Reduction of Atherosclerotic Cardiovascular Risk in Patients With Type 2 Diabetes. Circulation. 2022 Dec 13;146(24):1882–94.
- Lincoff AM, Brown-Frandsen K, Colhoun HM, Deanfield J, Emerson SS, Esbjerg S, et al. Semaglutide and Cardiovascular Outcomes in Obesity without Diabetes. N Engl J Med. 2023 Dec 14;389(24):2221–32.
- Kosiborod MN, Abildstrøm SZ, Borlaug BA, Butler J, Rasmussen S, Davies M, et al. Semaglutide in Patients with Heart Failure with Preserved Ejection Fraction and Obesity. N Engl J Med. 2023 Sep 21;389(12):1069–84.
- Karakasis P, Patoulias D, Fragakis N, Klisic A, Rizzo M. Effect of tirzepatide on albuminuria levels and renal function in patients with type 2 diabetes mellitus: A systematic review and multilevel meta-analysis. Diabetes Obes Metab [Internet]. 2023 Dec 20.
- Ida S, Kaneko R, Imataka K, Okubo K, Shirakura Y, Azuma K, et al. Effects of Antidiabetic Drugs on Muscle Mass in Type 2 Diabetes Mellitus. Curr Diabetes Rev. 2021;17(3):293–303.
- Wilding JPH, Batterham RL, Calanna S, Van Gaal LF, McGowan BM, Rosenstock J, et al. Impact of Semaglutide on Body Composition in Adults With Overweight or Obesity: Exploratory Analysis of the STEP 1 Study. J Endocr Soc. 2021 May 3;5(Supplement_1):A16–7.
- Wilding JPH, Batterham RL, Calanna S, Davies M, Van Gaal LF, Lingvay I, et al. Once-Weekly Semaglutide in Adults with Overweight or Obesity. N Engl J Med. 2021 Mar 18;384(11):989–1002.
- Reinmann A, Gafner SC, Hilfiker R, Bruyneel AV, Pataky Z, Allet L. Bariatric Surgery: Consequences on Functional Capacities in Patients With Obesity. Front Endocrinol. 2021 Apr 1;12:646283.
- Carlsson LMS, Carlsson B, Jacobson P, Karlsson C, Andersson-Assarsson JC, Kristensson FM, et al. Life expectancy after bariatric surgery or usual care in patients with or without baseline type 2 diabetes in Swedish Obese Subjects. Int J Obes. 2023 Oct;47(10):931–8.
- Wilding JPH, Batterham RL, Davies M, Van Gaal LF, Kandler K, Konakli K, et al. Weight regain and cardiometabolic effects after withdrawal of semaglutide: The STEP 1 trial extension. Diabetes Obes Metab. 2022 Aug;24(8):1553–64.
- Consumer trends: 2024 Food & Wellness special. The New Consumer. (n.d.). https://newconsumer.com/trends/consumer-trends-2024-food-wellness/
- Gorgojo-Martínez JJ, Mezquita-Raya P, Carretero-Gómez J, Castro A, Cebrián-Cuenca A, de Torres-Sánchez A, et al. Clinical Recommendations to Manage Gastrointestinal Adverse Events in Patients Treated with Glp-1 Receptor Agonists: A Multidisciplinary Expert Consensus. J Clin Med Res [Internet]. 2022 Dec 24;12(1).
- Tantawy SA, Kamel DM, Abdelbasset WK, Elgohary HM. Effects of a proposed physical activity and diet control to manage constipation in middle-aged obese women. Diabetes Metab Syndr Obes. 2017 Dec 14;10:513–9.
If you’re a coach, or you want to be…
You can help people build sustainable nutrition and lifestyle habits that will significantly improve their physical and mental health—while you make a great living doing what you love. We’ll show you how.
If you’d like to learn more, consider the PN Level 1 Nutrition Coaching Certification. (You can enroll now at a big discount.)
The post Ozempic for weight loss: What coaches (and clients) need to know about GLP-1 drugs appeared first on Precision Nutrition.
14 Jul, 2023 | Admin | No Comments
“Help! My client’s not losing weight despite claiming to follow a low calorie diet!”
Reviewed by Brian St. Pierre, MSc, RD, CSCS
“My client says they’re eating a super low calorie diet, but they’re not getting results… What should I do?!”
We see variations of the above “low-calorie-no-results” question in our Facebook coaching communities all the time. (“My client says they’re following 1200 Calorie diet, but…” or “My client’s weight hasn’t budged despite claiming to eat only 800 Calories per day…”)
Usually, about half of the respondents suggest the client is simply mistaken. “Nobody who says they’re eating that little actually is,” they say.
The other half center on biological problems that can slow someone’s metabolism: “You might suggest they visit their doc for a thyroid check-up.”
Both sides can be right.
But as a coach, how do you know how to proceed? What can you do if you or one of your clients is stuck in the low-Calorie-no-results cycle?
(And if your client really is eating more than they’re telling you: How do you bring it up—without calling them a liar?)
How to talk to clients about the “low-calorie-no-results” problem
Let’s start with a benchmark: For most women, a 1200 Calorie daily limit would create enough of a deficit to result in weight loss. For men, that number is about 1500 Calories.
This is true even if someone’s metabolism is running more slowly due to adaptive thermogenesis (or colloquially, “the starvation response”). It’s true for folks with thyroid issues as well.
Though there are health conditions that can theoretically slow someone’s metabolism enough to stop a 1200-Calorie diet from working, they are exceedingly rare, says Precision Nutrition Director of Nutrition Brian St. Pierre, MS, RD.
In other words, if your client is eating at or below the above calorie limits and still isn’t losing weight, a medical problem likely isn’t behind your client’s lack of results.
Much more likely, is this: Your client is eating more than they think they’re eating.
(Read more: Is a 1200-Calorie diet realistic?)
But your client isn’t “lying” to you.
It’s difficult to count calories with precision. On top of that, very low calorie diets are tough to follow consistently.
What happens is this:
Most people follow them consistently some of the time—and not at all at other times.
They might consume their intended calorie amount Monday through Wednesday.
On Thursday, they might get a little relaxed about their food choices, and unknowingly clock a few hundred extra Calories.
Then Friday hits and they go out to eat. A burger, some fries, and two beers later and they’re at well over 3000 calories—just for that day.
Splurge a little on Saturday too and there goes the weekly deficit.
From the client’s perspective, they’re following their intended diet.
They carefully limited calories Monday through Thursday-ish, and they also went to battle with many uncomfortable sensations, including hunger, cravings, and maybe some irritability.
“Yes, they’re providing you with false information, but they’re not doing it maliciously,” says Precision Nutrition Super Coach Kate Solovieva.
Instead, they might be afraid or ashamed to reveal what they’re eating, especially on those indulgent days when they go way over their target. Or, they may truly not remember those indulgences.
And yet, they’re still looking to YOU to solve what to them looks like a total mystery.
As you can imagine, this can require a tricky, sensitive discussion. Which is why we’ve created this 5-step process to help you through it.
(And if you’re still hungry for more communication strategies you can use to have better conversations with clients, read: Effective coach talk: What to say to clients and why it matters)
Step #1: Offer some validation.
Build trust and rapport by agreeing with your client’s perceived experience.
The opposite—calling them out on their math errors or high-calorie indulgences—might just make them feel defensive and even less likely to share openly with you.
You might say:
“It’s definitely unpleasant and uncomfortable to eat so little. It must be so frustrating to go through all of that and not see the scale move.”
Step #2: Create a “we’re in this together” vibe.
Forget the thought of dragging your client forward with a long lecture about how “there’s no way you’re eating 1200 Calories because….”
Instead, try to see yourself at the same level as your client by using “we” and “us” instead of “I” and “you.” This simple language shift will prevent you from saying resistance-triggering things like “you should…” and “what you need to do…”
You might say:
“Let’s put on our detective hats and figure this out together. To solve this mystery, we’re going to need to gather some data. This will help us see what’s impeding fat loss.”
Step #3. Gather some data.
Ask your client to track everything they eat for two weeks.
But before you start, remember that most clients want to impress their coaches. As a result, many people don’t track when they feel guilty or ashamed about what they’ve eaten, explains Solovieva.
So, encourage your client to consider any data they record as just that: data. Not a proxy for their value as a person, or as a measure of their “goodness.”
You might say:
“How do you feel about keeping a detailed food diary for two weeks? I’m suggesting this because it’ll help us determine what’s up. And I know this is uncomfortable, but it’s also really important to track the things you don’t want me to see. I promise: I won’t judge. Eat a whole pizza? Four margaritas? No judgment. If we gather accurate information, then we can have a better idea of what to do next.”
Step #4: Look at the numbers together.
After two weeks of tracking, you’ll likely notice one of the following trends.
 Outcome A: The scale is moving.
Outcome A: The scale is moving.
Because they knew you’d be looking at their log, your client felt more accountable. As a result, they ate their intended calorie intake consistently, seven days a week.
Ask your client how they feel.
If they report unbearable hunger, fatigue, and cravings, you might say, “Okay, that’s telling me that your body will lose fat on a 1200-Calorie diet. That said, it’s also telling me that this might not be a good strategy long-term.”
Then proceed to step 5.
Outcome B: There are gaps in your client’s food log.
Let’s say Monday through Wednesday are complete. But Thursday through Saturday are blank.
In this case, you might say, “I see you didn’t fill out your log for a few days. What was happening on those days?”
As your client talks, avoid jumping in with your own conclusions. Instead, gently ask questions—being curious and non-judgmental—to help your client reveal the full story.
If your client does indeed tell you they might’ve eaten a bit more on those days, you can simply say, “Sure, it’s really tough to maintain such a big calorie deficit. Given what you told me though, how do you think we should interpret our data this week?”
Then move to step 5.
Step #5: Try an experiment.
Here’s a great coaching trick if you feel like your client is rebelling against or just struggling with an advanced dietary strategy—like following an ultra low-calorie diet:
Frame whatever you try as an “experiment.”
Say, “Let’s look at what we can do to make this easier and most sustainable. How do you feel about trying an experiment? It would just be for two weeks. If it doesn’t work, we can try something else.”
Then suggest one of the experiments below.
Experiment #1: Eat more.
Instead of 1200 Calories, suggest your client consume 1500.
(If they’re not starting at 1200 Calories, just add a few hundred calories to whatever their original intended caloric intake was.)
You might say, “What if we try eating a little bit more? It’s just an experiment, so if it doesn’t work, we can always go back. But you’ll still be in a deficit, so you should still make progress. It’ll just be more tolerable.”
No matter how you word things, some clients will still say, “No way.” In that case, follow up with, “How about we meet in the middle. How does 1350 Calories sound? Let’s just test it for two weeks.”
Experiment #2: Track calories—but without a calorie target.
This experiment helps to build the skill of tracking accurately, says Solovieva.
Tell your client:
“This isn’t about changing what or how much you eat. Instead, all I want you to do is write down what you eat. What we’re trying to do is build the skill of tracking accurately and consistently. Know that there will be times when you’ll want to avoid tracking—possibly because you don’t want me to see what you ate—but that data is important. And remember, I won’t judge.”
After a couple of weeks of doing this, your client will probably have some revelations: like how many calories are really in that scoop of peanut butter, how many times they tend to “sneak” food and pretend it doesn’t count, or how much food they tend to eat when they’re not trying to control or limit their intake.
With this information, clients can then better assess how many calories they’re willing to cut, and where pitfalls might happen.
Experiment #3: Forget calorie tracking.
Sometimes you have to completely step away from one strategy to create the time and energy for a more effective one, says Solovieva.
If calorie-tracking isn’t working, stop doing it—and try something else.
You can say, “You know, maybe the calorie tracking thing isn’t working right now. How do you feel about a different approach?”
Then suggest a—hopefully more manageable—action such as tracking:
- Grams of protein
- Servings of vegetables
- Hunger and fullness metrics
Or, the client can focus on a completely different behavior, such as bumping up their exercise minutes or eating slowly.
(And if your client thinks eating slowly sounds like a skill for sissies, get them to check out: The 30-day eating challenge that can blow your mind—and transform your body)
What to do when clients consistently track inaccurately
Clients don’t hide or mess up data because they’re trying to vex you.
“More likely the client is worried about upsetting you,” says Solovieva. “They already feel ashamed, and they assume you’ll say or do something to make them feel even worse.”
To circumvent this problem, use this advice.
Look in the mirror.
Consider: Why doesn’t your client feel comfortable sharing everything? Is it possible you might have contributed? Get honest about the stories you hold about your client. Unspoken thoughts like “They’re lying” or “They’re lazy” can come through in your vibe, voice, and tone, says Solovieva.
Respect your client’s silences.
If they don’t say anything when you ask about a gap in the log, it’s a sign they’re deeply uncomfortable talking about it. In that case, just move on. Don’t try to pry the information out of them, Solovieva says. When they’re ready, they’ll share.
Don’t demonize food or people.
Clients will test you, especially in the beginning of the coaching relationship, to see how you’ll react, says Solovieva. For example, they might tell you about a friend who eats donuts for breakfast—but they’re really talking about themselves. If you take the bait and respond critically, you ruin your chances of them being more open and honest with you in the future.
Sit on the same side of the desk.
It’s often overlooked, but our environments can shape how comfortable we feel, and the way we interact with each other. For example, if you typically sit behind a big desk, that barrier can easily make it feel like you’re an authority figure and your client is your subordinate, says St. Pierre. Play around with different configurations. Sitting side-by-side, or slightly angled toward one another, can facilitate more of a peer-to-peer vibe that can be more conducive to sharing openly.
Forget about calling people out.
Even if you do everything we’ve suggested above, you’ll likely encounter clients who say they want to stick to a low-calorie diet no matter what, despite turning in food logs, week after week, that don’t list everything they ate.
You’ll know this because, on Instagram, they’ve posted a photo of themselves and a huge burger—that isn’t on their log.
You might be tempted to lecture.
However, sometimes saying nothing can be more effective than saying something.
As Solovieva says, “Calling out tends to elicit shame—and more shame has never led to more change.”
Allow your clients their defense mechanisms and their human errors. What’s most important is that you foster a trusting, positive relationship with them. With that kind of unconditional support, most clients will eventually open up, and be willing to look at realistic ways they can change—and improve.
If you’re a coach, or you want to be…
You can help people build sustainable nutrition and lifestyle habits that will significantly improve their physical and mental health—while you make a great living doing what you love. We’ll show you how.
If you’d like to learn more, consider the PN Level 1 Nutrition Coaching Certification. (You can enroll now at a big discount.)
The post “Help! My client’s not losing weight despite claiming to follow a low calorie diet!” appeared first on Precision Nutrition.
14 Jul, 2023 | Admin | No Comments
Is a 1200-Calorie diet (or any super low-calorie diet) actually realistic?
Reviewed by Brian St. Pierre, MSc, RD, CSCS
If Jerry Seinfeld were into health and fitness he’d ask, “What’s the deal with the 1200-Calorie diet?”
(Thanks for the joke, Dad.)
But seriously: If you look at the caloric recommendations of many popular weight loss diets, you’ll notice that 1200 Calories is often the “ideal target” for women. (For men, it’s often 1500.)
The 1200-Calorie diet is also an extremely popular topic on Reddit, TikTok, and Instagram. Allegedly, even Kim Kardashian followed this prescriptive diet.
There’s nothing special about 1200 Calories specifically.
However, all this hype makes a person—or a concerned coach—wonder about low-calorie diets in general.
Most importantly: Is such a low caloric target safe and sustainable?
In the following article, we’ll address that question, as well as:
- Why some people don’t lose weight on 1200–Calorie diets. (Hint: It has nothing to do with their thyroid or metabolic adaptation.)
- The daily calorie target that tends to stimulate weight loss—and not unbearable cravings or deprivation.
- Four science-supported strategies that help regulate appetite and hunger—so folks can follow their food plan for the long term.
But first…
Where did the 1200-Calorie diet come from, anyway??
It’s thought that the 1200-Calorie Diet dates back to 1918, when Lulu Hunt Peters, MD, released a book titled Diet and Health with Key to the Calories.
Dr. Peters writes in an entertaining manner, which may be what led to the book’s lasting popularity. In 2005, the book was reprinted digitally, more than 80 years after its initial release and long after Dr. Peters’ death.
For example, within its pages, you’ll find lots of messy stick and circle figures, along with advice to “skip this chapter. It will not interest you in the least.”
Among the book’s prescriptive advice, readers are cautioned against consuming too much animal protein, as it “makes the disposition more vicious.” For exercise, Dr. Peters encourages women to brush their hair vigorously, “at least 200 double strokes all over the head.”
(Not everything from this book survived the test of time.)
Embedded throughout is encouragement to consume 1200 Calories. (Says the book: “You will be surprised how much 1200 Calories will be if the food is judiciously selected.”)
Dr. Peters’ thinking—as well as the thinking of today’s 1200-Calorie diet proponents—goes like this:
- Most women need about 2200 daily Calories to maintain their weight.
- A pound of fat contains 3500 Calories.
- If you consume 1000 fewer daily Calories than you need, you will lose about two pounds of fat a week. (Because math.)
Thing is, while the arithmetic is straightforward, fat loss is anything but.
Because—quick fact check—not all women’s total daily energy expenditure (TDEE) will be 2200 Calories. A woman’s calorie needs will depend on many factors, including her body size, lean mass, age, dieting history, and activity levels.1
TDEE might be much higher than 2200 for some women and much lower for others.
In other words, 2200 Calories is an average—and not a universal number that applies to all women.
Why some people don’t lose weight on a 1200-Calorie diet
Very low calorie diets can and do lead to fat loss—if you stick to them, consistently.
For many women, 1200 represents about half the calories they need to maintain their weight. That’s enough of a deficit to lead to weight loss for most people, including folks with thyroid problems.
It can even overcome adaptive thermogenesis—or the “slowing” of the metabolism after an extended period of caloric deficit. (Colloquially, this is what some folks call “the starvation response.”)
We know about this because of research done almost 80 years ago.
How your body fights back against the 1200-Calorie diet
In the mid-1940s, University of Minnesota researchers published a study called “The Minnesota Starvation Experiment.”
In this study, 36 men voluntarily semi-starved themselves for six months—all in the name of science. The men ate 1570 daily Calories from food carefully portioned by dietitians. The meals added up to half their normal intake.
Interestingly, their basal metabolic rates did drop—by a whopping 40 percent—but it didn’t stop them from losing weight. After six months, every single one of the men had lost about 25 percent of their weight—no exceptions. 2, 3
Problem is, semi-starvation is brutal.
The longer you sustain such a severe calorie deficit, the more your biology fights you, turning down metabolism and turning up hunger and cravings.
(Your body wants you to survive the famine!)
As a result, you may find—as the men in the Minnesota starvation study did—food becomes all you talk about, think about, and dream about.
Food preoccupation became so intense for the Minnesota men that they would routinely lick their plates clean after meals, and even rummage through the trash for food scraps between meals.
(Many of these behaviors persisted even after the study ceased. Study alumni reported needing to keep snacks with them at all times, so they would never have to worry about hunger again.)
During sustained caloric deprivation, many other biological chemicals get out of whack, too, leading to more headaches, depression, anxiety, and cold intolerance.
Plus, your ability to concentrate drops, mostly because you can’t focus on anything other than “WHEN’S MY NEXT MEAL???”
At this low calorie amount, it’s also difficult to consume enough food to meet all your nutrient needs, too. So, the risk of malnutrition goes up.
How the 1200-Calorie diet often fails
Because of everything we mentioned above, it’s difficult to consume 1200 Calories day after day.
Instead, what usually happens: Folks nail their calorie targets some days, and wildly exceed it on others.
“Clients say ‘I’m eating 1200 or 1300 Calories a day.’ That’s usually true-ish,” says Brian St. Pierre, MS, RD, Precision Nutrition’s Director of Nutrition. “They’re in the ballpark four to five days a week.”
On the other days, however, dieters find themselves drawn to highly indulgent, calorie-dense foods like…
- A whole pizza, plus two beers (2200+ Calories)
- A burrito, two margaritas, chips, and guacamole (2000+ Calories)
- A gourmet burger with fries and a cola (1500 Calories)
- Pasta with chicken and roasted garlic from The Cheesecake Factory (1910 Calories)
Even if you’re following your regular low-cal diet for most of the day, just one of the above meals can push your daily total well above 3000 Calories.
A so-called cheat day can also add multiple thousands of calories to your weekly total. Yes, you consumed 1200 Calories on many days—but your daily caloric average may be north of 1800.
Depending on your body size and activity level, that may mean no—or just very slow—fat loss.
Even if weight loss is happening, people’s expectations—especially when they’re acutely miserable eating 1200 Calories 4 or 5 days a week and think weight should be free-falling off—can set them up for disappointment.
(Talking to clients who are frustrated with their results despite claiming to eat a low-cal can be a tricky, sensitive conversation. For help, check out the 5 steps outlined here: “Help! My client’s not losing weight despite claiming to follow a low calorie diet!”)
3 types of clients who might do well on a 1200-Calorie diet
We just made very-low-calorie diets sound like the big bad wolf.
But the truth is, they can be appropriate for some people like:
► Small women: Someone who stands 4 feet, 10 inches tall, weighs 110 pounds, and doesn’t exercise might consume 1200 Calories to maintain or lose a small amount of weight.
► Clients adept at advanced nutrition protocols: “If you get paid to look a certain way during a specific time frame, you’re often more comfortable with the tradeoffs,” St. Pierre says.
These clients—like weight-classed athletes, figure competitors, or celebrities—tend to use ultra low-calorie diets as a temporary tool.
Along with water weight manipulation (and maybe some spray tanning/contouring and good lighting) extreme “cuts” can get these clients competition or photo-shoot ready.
After the big day is over, they return to a more sustainable calorie target.
► Bariatric patients: The 1200 Calorie target might also make sense for someone who needs to lose weight rapidly for health reasons. Dr. Nowzaradan—one of the stars of the TV show “My 600-Lb. Life”—famously recommends 1200-Calorie diets for his patients.
In this case, the person should undergo the diet under the direction of a medical professional.
(There’s lots of misconceptions around low-calorie diets. If you’re interested in understanding how they really affect your body, read: Can eating too little damage your metabolism?)
A better way to lose fat—and keep it off.
One solution to the 1200-Calorie dilemma is counterintuitive: Bump your daily target up to around 1500 Calories, says St. Pierre.
(For men: Go higher, to around 1800, depending on your activity level and body size.)
You might wonder: ‘If I (or my client) wasn’t losing weight on a 1200-Calorie diet, how could I possibly lose weight by eating… MORE? Shouldn’t I eat even LESS?’
Here’s why it works: By adding just a few hundred daily calories, you’ll reduce the intense hunger, cravings, fatigue, and food obsessions that make it so difficult to remain consistent.
“It feels as if you’re eating more because, on most days, you are,” says St. Pierre.
“Yet, while you’ll eat more each day with 1500 Calories, you’ll likely consume less each week.” The chart below shows how.
(Note: Because no one consumes the exact calorie amount—day after day—we’ve varied the daily calories to make them more realistic.)
| Aiming for 1500 Daily Calories | Aiming for 1200 Daily Calories | |
| Monday | 1520 | 1205 |
| Tuesday | 1480 | 1180 |
| Wednesday | 1510 | 1215 |
| Thursday | 1490 | 1900 |
| Friday | 1515 | 3200 |
| Saturday | 1485 | 2800 |
| Sunday | 1505 | 1180 |
| Weekly total: | 10,505 | 13,280 |
| Daily Average: | 1500 | 1811 |
However, even after bumping up daily calorie allowances, some people may still struggle with intense hunger and cravings.
So, here are four strategies that make maintaining a calorie deficit a little more comfortable, and make fat loss more sustainable.
1. Include lean protein at every meal.
Protein takes longer to digest than carbohydrates or fats. It also stimulates the release of hunger and appetite-suppressing hormones like cholecystokinin (CCK) as well as drives down levels of the hunger hormone ghrelin.
According to a scientific theory known as the protein leverage hypothesis—often referred to as “protein hunger” in lay circles—the human body will keep hunger and appetite fired up until basic protein needs are met.
(Note: There’s conflicting research on this hypothesis… which is why it’s still termed a hypothesis—and not, say, a law.)
Eat mostly low protein foods and you’ll likely remain frustratingly hungry, even though you’ve consumed a lot of calories. 4
(See our “What Should I Eat?!” infographic for the best protein sources.)
How to do it:
Aim for at least 4-5 palm-sized portions of lean protein daily.
Try to spread your intake out relatively evenly, consuming 1 to 2 palm-sized portions during every meal and snack.
High protein sources include fish, shellfish, chicken, turkey, beef, eggs and egg whites, cultured cottage cheese, unflavored Greek yogurt, tofu, tempeh, seitan, and protein powders.
2. Increase your intake of non-starchy veggies.
If you ate an entire head of cauliflower, you’d likely feel as if you were walking around with a brick in your stomach.
Yet, you’d only have consumed 146 Calories, give or take.
Compare that to the half slice of pizza you’d get for the same number of calories and you can understand why non-starchy veggies can help with fat loss.
Loaded with water and fiber, veggies offer tons of volume for very few calories.
According to the Nurses Health Study, which tracked the health outcomes of 133,000 people over several decades: Every additional daily serving of veggies (and fruits too, for that matter) was associated with a drop in weight. 5
How to do it:
Gradually increase your daily veggie target over time, aiming for at least 4 fist-sized servings a day (along with 2-3 cupped handfuls of fruit). This increases the volume of food you eat without spiking caloric intake, so you can feel more satisfied with less.
Of course, sometimes an order of fries or a slice of pizza is worth it—yes, even instead of carrot sticks or a salad entree.
Likely, the best meals are built with plenty of vegetables and lean protein to help you feel full and satisfied and small to moderate amounts of the really delicious mouth-happy foods that bring you pleasure.
3. Gravitate toward minimally-processed whole foods.
When people reduce calories, they sometimes lean hard into pre-packaged foods that are marketed for weight loss, such as sugar-free pudding cups, packaged diet bars, fat-free hot dogs, low-carb bread, and diet shakes.
“These kinds of foods aren’t usually satisfying,” says St. Pierre.
First, they don’t taste particularly great, so they often leave you yearning for the real, full-fat, full-carb, full-sugar deal.
On top of that, they lack key nutrients—especially protein and fiber—that help keep hunger and appetite in check.
By shifting away from highly-processed foods and “diet foods” and toward minimally-processed whole foods, you’ll automatically consume more fiber, protein, vitamins, minerals, and phytochemicals.
End result: You’ll feel less hungry and more satisfied.
How to do it:
Start by making small swaps.
For example, maybe you’re a chip-lover, and you tend to reach for them (and reach again) when you’re hungry between meals.
Now think: What’s a minimally-processed food that you like and would even look forward to eating, that you could keep accessible during those snack-attacks, so you have an alternative to chips?
Chances are, that choice is also going to end up being more nutritious and satiating—while also being lower-calorie, partly because it’s harder to overeat minimally-processed foods. (Unlike chips! [shakes fist])
Sounds simple, but we’ve seen people dramatically transform their diet over time with this approach—with way less effort than people who simply try to restrict their food intake.
When you’re ready, you can do other swaps, gradually increasing your intake of minimally-processed whole foods until they compose most of your diet.
(For ideas on how to make these relatively painless swaps, check out this piece: Meal plans usually suck: Here are 6 better ways to transform your diet)
In our experience, most people can find an excellent balance between health and pleasure when minimally-processed foods comprise roughly 70 to 80 percent of their overall diet.
(If you’re curious about the many other reasons highly-processed foods make you feel like you always need MORE, check out: Why you can’t stop overeating junk food.)
4. Add resistance training.
Usually, weight loss comes from a combination of fat loss and muscle loss.
Muscle loss, however, is associated with an increase in the hunger hormone ghrelin and the appetite hormone insulin-like growth factor (IGF).
Basically, your body is trying to maintain muscle mass, so it’s turning up hunger and appetite in order to nudge you to eat its building blocks.
Though strength training doesn’t 100 percent eliminate muscle loss during weight loss, it can preserve most of it.
That’s key because, according to recent research, preserving lean mass may help blunt at least some of the appetite and hunger increases folks experience as they lose weight. 6
How to do it: If you’re not doing it already, add a twice-weekly strength training session to your routine, following a program that targets all of your major muscle groups.
(If you’re just getting started with strength training, consider downloading our FREE 14-day at-home workout program.)
The honest truth: Some hunger is inevitable.
Anyone who tells you that you can “lose weight without hunger” is likely trying to sell you something.
If you follow the 1200 Calorie Diet—or just consume fewer calories than your body is used to—your body is going to toss up a hunger flare.
That said, if you…
- Slightly bump up your overall calorie intake
- Optimize your consumption of lean protein, veggies, and whole foods (while still allowing some “just for pleasure” treats so you don’t feel deprived)
- Incorporate regular strength training
… You’ll be able to lose fat without feeling exceptionally hungry and deprived—and even keep it off.
“You’ll feel more satisfied, you’ll mentally feel better, and you’ll physically feel better,” says St. Pierre. “You can still make progress, just in a way that sucks a lot less.”
jQuery(document).ready(function(){
jQuery(“#references_link”).click(function(){
jQuery(“#references_holder”).show();
jQuery(“#references_link”).parent().hide();
});
});
References
Click here to view the information sources referenced in this article.
- Pontzer H, Yamada Y, Sagayama H, Ainslie PN, Andersen LF, Anderson LJ, et al. Daily energy expenditure through the human life course. Science. 2021 Aug 13;373(6556):808–12.
- Kalm LM, Semba RD. They starved so that others be better fed: remembering Ancel Keys and the Minnesota experiment. J Nutr. 2005 Jun;135(6):1347–52.
- Tobey JA. The Biology of Human Starvation. Am J Public Health Nations Health. 1951 Feb;41(2):236.
- Grech A, Sui Z, Rangan A, Simpson SJ, Coogan SCP, Raubenheimer D. Macronutrient (im)balance drives energy intake in an obesogenic food environment: An ecological analysis. Obesity. 2022 Nov;30(11):2156–66.
- Bertoia ML, Mukamal KJ, Cahill LE, Hou T, Ludwig DS, Mozaffarian D, et al. Changes in Intake of Fruits and Vegetables and Weight Change in United States Men and Women Followed for Up to 24 Years: Analysis from Three Prospective Cohort Studies. PLoS Med. 2015 Sep;12(9):e1001878.
- Turicchi J, O’Driscoll R, Finlayson G, Duarte C, Hopkins M, Martins N, et al. Associations between the proportion of fat-free mass loss during weight loss, changes in appetite, and subsequent weight change: results from a randomized 2-stage dietary intervention trial. Am J Clin Nutr. 2020 Mar 1;111(3):536–44.
If you’re a coach, or you want to be…
You can help people build sustainable nutrition and lifestyle habits that will significantly improve their physical and mental health—while you make a great living doing what you love. We’ll show you how.
If you’d like to learn more, consider the PN Level 1 Nutrition Coaching Certification. (You can enroll now at a big discount.)
The post Is a 1200-Calorie diet (or any super low-calorie diet) actually realistic? appeared first on Precision Nutrition.
12 Jan, 2023 | Admin | No Comments
Level 1: The “Deep Health” coaching secret that transforms short-term fitness goals into life-changing results
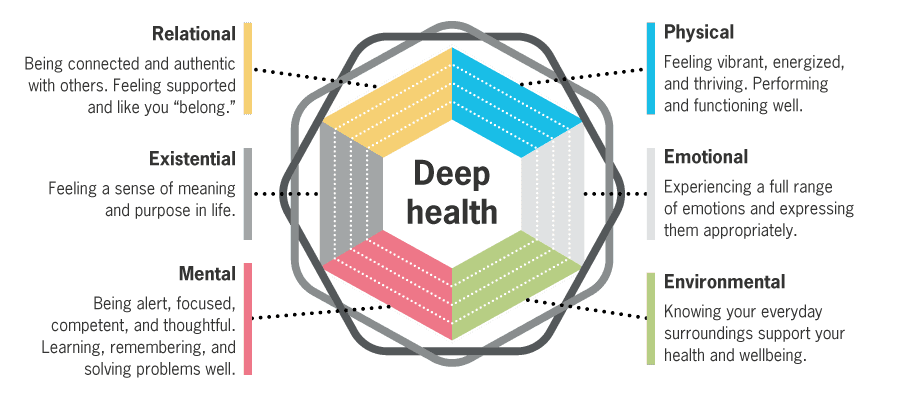
Losing 10 pounds. Running a half marathon. Getting six-pack abs. How do you turn short-term client goals into something meaningful, sustainable, and inspiring? Enter: Deep Health coaching, the revolutionary method that gets your clients the results they want, plus the results they need.
++++
Are you truly transforming your clients’ health?
Are you helping them thrive, in all aspects of life?
Sure, you may be helping them boost their bench press, feel confident on their beach vacation, or get sidewalk-cracking swole.
But what if we told you food and fitness—the domains of physical health—are only 16 percent of what determines your clients’ success?
What if you could move beyond “12 week beach bod programs,” or “pre-wedding weight loss,” to something truly meaningful and sustainable, and even more inspiring?
After all… what happens to the beach bod at week 13?
Or by the 10th wedding anniversary?
Can your clients stay at or even grow beyond their goals without feeling deprived, hungry, and miserable?
Without turning food and fitness into a full-time job?
And without backsliding from short-lived pride and mirror selfies into enduring shame and baggy sweatshirts?
Is there a way that YOU can build a sustainable coaching business where you continually help people learn, grow, and improve… without having to constantly hustle new clients or start from scratch over and over?
Where your clients aren’t just okay with the quick-fix results they get… but transformed inside and out, to the point where they rave about you to their friends and family?
What if you could be a coaching alchemist… someone who turns superficial physical goals into substantive life gold?
After working with over 150,000 clients, we believe you can get more ambitious—and be more effective and fulfilled—with an approach that goes far beyond the superficial.
It’s called coaching for Deep Health.
This is when all dimensions of health are in sync, instead of just the physical.
It’s not only about how your clients look or perform.
It’s also about how they think, respond, solve problems, and deal with the world around them.
“Wait,” you might say. “I’m all for Deep Health, but my 4pm is here and they want to lose 20 pounds.”
Perfect.
Coaching for Deep Health will help you get them there faster and more easily than ever before—in a way that fits their life and is sustainable.
(That’s good for your clients.)
Their results will translate into glowing reviews, lots of referral business, and an invaluable sense of career fulfillment.
(That’s good for you.)
++++
The six dimensions of Deep Health
Deep Health doesn’t come from a pill or an operation.
Deep Health comes from a balanced diet of fresh, whole foods. It comes from sufficient exercise combined with genuine rest. It comes from fresh air and clean water. It comes from real human connection and sincere emotional expression.
And it comes from living with purpose and joy, and using your life as an expression of these things.
When you coach for Deep Health, you consider the multi-dimensional thriving of a whole person in their whole life.
Not just body fat percentage and blood work, but also factors like how people think, feel, live, and connect to others.
Don’t worry: We’re not suggesting you master psychotherapy, or tackle the human condition.
We are suggesting you understand how healthy eating and lifestyle practices affect every aspect of your client’s well-being. And how every dimension of Deep Health affects the eating and lifestyle practices of your clients.
Here are the six dimensions of Deep Health.
These areas of health are deeply entwined and strongly connected.
You probably know how we feel can affect how we eat. (This is, after all, most people’s #1 nutrition challenge.)
You might have also noticed that people with supportive families, strong connections at their gyms, or welcoming fitness communities (such as running or cycling groups) are more likely to show up for their workouts.
Or that people with a clear purpose, self-stories that foster healthy activities, or the willingness to change suffering into action are more likely to stay motivated and succeed.
Every dimension of Deep Health influences eating and exercise behaviors.
That’s what coaching for Deep Health is all about.
Let’s see how this might look in real life.
Example 1: Your client is a dedicated runner with an injury.
They can’t run properly, which means they can’t train, and they’re getting deconditioned. That’s the current state of their physical health.
But because of this situation, they’re also:
- feeling depressed and frustrated (emotional health)
- lonely and disconnected, missing their weekend run clubs and races (relational health)
- starting to wonder what the point of anything is (existential health)
Example 2: Your client works long hours at a high-stress job.
They sit at a desk (which affects their physical health via inactivity and back / neck pain), and they don’t get their proper sleep (physical health impact again).
Because of this situation, they’re also:
- anxious and stressed, answering emails late at night (emotional health)
- arguing with their partner about working too much (relational health)
- spending most of their time in a windowless cubicle with takeout food a phone call away (environmental health)
- on the cusp of a midlife crisis (existential health)
Now… here’s the really cool part:
The problems are connected… but so are the solutions.
Struggling in one dimension of deep health usually means struggling in others.
But there’s a flip side here, too.
Improving one dimension can also improve others.
This is the power of Deep Health coaching.
Maybe you help your injured client find alternative activities and mentally manage their pain.
For instance, you might introduce them to water sports or swimming. You help them normalize injury and work on rehab.
They get back to movement. They feel happier. They meet new friends at dragon boating or the local pool.
Or, maybe you give your stressed-out client some relaxation techniques, a bit of mobility work to do at their desk, and the number of a healthy meal delivery service. Plus, you empathize with their challenges.
They calm down a little, move more in their day, concentrate better, and (as a result of better focus and hence productivity) even find time to come home half an hour earlier, which makes their spouse happier.
Winning!
Pull a lever in one dimension of Deep Health, and gears in other dimensions will also move.
Use the connections between Deep Health dimensions to your advantage. If one area is off-limits or temporarily broken, try another one.
Deep Health looks different for everyone.
For a young stay-at-home parent, it could be balancing a certain pants size with weekly ice cream night with their kids.
For an elite powerlifter, it might be pushing their bench press without screwing up their shoulders or social life.
For a retiree in their 70s, it may be “mobility over medication”—staying off the blood pressure pills and enjoying long walks with their spouse.
That’s why your clients need coaching that’s individualized and thoughtful.
Deep Health isn’t about rules or ideals.
It’s about exploration and invitation.
Explore your clients’ worlds to find areas for growth, improvement, and learning. Then, invite them to do that growth and learning along with you.
This offers you unlimited coaching possibilities… and a long-term, lucrative and fulfilling coaching relationship for both client and coach.
Coach for Deep Health… and better results
Where do you start?
Easy… just ask your clients.
They can tell you where they need the most help, or where they want to flourish more.
Don’t think of this process as a diagnosis or an interrogation.
Instead, think of it more like opening a conversation, building a story, and deepening a coaching connection.
You can casually ask one of these questions, or all of them, if you want.
You can ask and intuit in various ways, gathering data from a range of client cues (for instance, their body language).
You can even make these questions part of your progress check-ins, if you like, using our free Deep Health Assessment tool below.
![]()
© Precision Nutrition
Often, this simple awareness is enough to spark a conversation about change.
Or, you can guide clients more deliberately towards noticing what might need their attention. (Example: “I find that clients who have trouble sleeping also have trouble managing their appetite… Does that feel true for you?”)
Of course, as you probably know, telling clients what to do doesn’t work. So instead of evaluating your client’s Deep Health Assessment and giving them an “assignment,” ask them:
“What’s on your garbage list?”
These are behaviors you know are total “garbage” for your health, sanity, and well-being—but you do them anyway. Everyone’s got a few.
Weekend overeating, skipping recovery days, and not getting enough sleep are some of the most common garbage list items. But they could also be anything from engaging in negative self-talk to stocking the freezer with ice cream every Friday.
Asking about a client’s garbage list is a quick-and-dirty way to figure out where to prioritize your efforts, and get them on the path to Deep Health.
But it’s only just the beginning.
If you want to start to truly master this coaching philosophy, read on.
Ask the right questions… to find mind-blowing solutions.
After the initial assessment, you’ll probably have a good working hypothesis about your client’s Deep Health.
So as a coach, you have two roles to play at this point:
Deep Health detective: Investigate.
- In which area(s) does it seem like there may be more to uncover?
- Where is your client struggling most?
Deep Health sherpa: Guide.
- Don’t “fix,” but enhance your client’s awareness.
- Collaborate to explore where they can seek help—or come up with their own solutions (with some supportive coaching).
In short: Let your client tell you what they need in order to see results.
Below is a handy quick-start conversation guide to help you accomplish that. There are a couple ways to use it.
Option 1: Work your way through each question, searching for places where you want to dig deeper. In those areas, use the follow-up questions to find out more.
Option 2: Skip right to the question that pertains to the area where your client needs the most help. Use the initial question to start a conversation, then dive into the follow-up questions to get more detailed.
In both cases, you can use the “action-focused thinking” questions to help your client start brainstorming solutions.
They don’t have to make any decisions about how to change things right away, but these questions will help get the process started.
Deep Health Dimension #1
Physical health: “How do you feel physically?”
Sometimes people can tell you clearly and specifically about their food, exercise, health, mobility/pain, and overall recovery.
For instance, maybe they’ll say “I’m freaking exhausted because I work 12-hour shifts. My knees hurt from lots of standing on the job. I have no energy to cook, and so I eat convenience-store crap.”
Great! Now you have a solid direction.
Sometimes they can’t tell you what’s up. Or they’ll say “Meh, okay, I guess.”
If that happens, no problem. Try some of the follow-up questions below and see what your client says. If you’re not making progress, you can always focus on a different area.
Potential follow-up questions
- Learn more about nutrition struggles: “What’s your biggest nutrition challenge right now?
- Find obstacles to movement: “How do you feel when you exercise?”
- Action-focused thinking: “What’s keeping you from getting the body you really want?”
Deep Health Dimension #2
Emotional health: “How are you doing emotionally?”
This can be difficult to talk about, but it matters. How your client feels emotionally on a day-to-day basis can impact everything from their nutrition habits to their relationships with others.
A quick pro tip: For many of these questions, what your client doesn’t say is almost as important as what they do say.
Look for body language cues, especially if they’re telling an emotionally laden story. Like, if they smile rigidly while saying “I want to kill my boss,” or seem to collapse like a pile of unwashed laundry while saying “I’m so discouraged with my performance.”
If they give you a one-word answer, consider pressing further. Maybe there’s nothing there, but you won’t find out unless you ask.
Potential follow-up questions
- Understand their ability to deal with emotions: “Sounds like you had a pretty bad day yesterday. How did you deal with that?”
- Evaluate general mood: “If you had to describe your overall mood in three words, what would they be?”
- Action-focused thinking: “What do those three words [above] tell you? Is there anything you’d like to change about your emotional health?”
Deep Health Dimension #3
Mental health: “What happened last time you were presented with a big logistical challenge?”
This area is mostly about how well their mind is working. And this question helps clients evaluate their ability to problem-solve, focus, prioritize, and put things in perspective.
You’ll also get a chance to see what their capacity for insight is like. Do they offer any additional reflections about how they handled the situation? Or how they could have handled the situation differently?
A client who’s not doing so hot in this area could be having a hard time focusing at work or constantly forgetting important items on their to-do list. So keep an eye out for signs they could benefit from upping their mental game.
Potential follow-up questions
- Search for gaps in organization and mental clarity: “How do you keep track of all the things you have to get done in any given day?”
- Assess creativity: “Where and when do you have the best ideas?”
- Action-focused thinking: “What do you think you need in order to have a clearer head?”
Deep Health Dimension #4
Existential health: “Why do you want to make changes to your health?”
Existential health refers to having a deeper “why,” or feeling like our actions have meaning.
When we have a strong sense of ourselves and what we’re here to do, we feel worthwhile. Valuing ourselves then affects how we treat our minds, our bodies, and the people around us.
People find meaning in roles as varied as being the best parent they can be to making the world a better place through their work. The important thing is that your client finds meaning in something.
Clearly understanding motivations, or what’s driving the desire to change, is also important. We can change without knowing exactly why we’re doing it, but it helps to feel like there’s a deeper purpose to the discomfort we’re facing.
And just a heads up, the more times you offer a curious “why?”, the more likely you are to get to the real reason they want to make a change in their life. Practice starting sentences with “I’m wondering about…” and “Why…?”
Potential follow-up questions
- Look for overall purpose: “What’s driving you, here? What’s lighting a fire under your butt to do this, or live life in general?”
- Ask about the “not-why”: “What’s not driving you? What do you not care about doing or having?” (Sometimes it’s easier for people to name what they don’t want, then you can explore the opposite to uncover what they really value.)
- Gauge their sense of belonging: How do you see yourself fitting into the “big picture?”
- Action-focused thinking: “What do you think would give your life more meaning? Is there anything you already do that you find meaningful?”
Deep Health Dimension #5
Relational health: “Who in your life is supporting you in this health journey?”
Social support is incredibly important to success in a health and fitness journey, so finding out if your client has it can help you better assess their needs.
If your client has someone in mind they know they can rely on for support, it’s a good exercise for them to “notice and name” that person. This question may also help your client realize they need to ask for support from someone close to them, like a partner or spouse.
Relationships may affect your client’s habits without them even realizing it. For example, if their partner prefers to watch TV while eating dinner, it may be more difficult for them to eat slowly and concentrate on their food.
Potential follow-up questions
- Probe for meaningful relationships: “It sounds like Person X really matters to you! Can you tell me more about how they support you?”
- Gauge their sense of belonging: “Where and with who do you feel like you ‘belong?’”
- Action-focused thinking: “What do you need from the people you’re close to in order to succeed?”
Deep Health Dimension #6
Environmental health: “How do your surroundings affect your health?”
Everything from the food in your house to the weather in your city to the political atmosphere in your country is part of your environment.
Being and feeling safe, secure, and supported by your environment enables you to make better choices for your health.
Having access to resources such as healthcare or healthy food is also part of environmental health.
We can’t control some elements of our environment. They’re more structural and systemic, woven into the fabric of our societies. These are called social determinants of health, and include poverty, racism, homophobia, lack of accommodation for disabilities, and displacement (as in the case of refugees).
In any of these situations, it may be very difficult to take steps to change someone’s environment. What can help is to focus on the things you can control wherever possible.
Potential follow-up questions
- Determine access to resources: “Is there anything you feel you need in order to reach your goals that you don’t currently have access to?”
- Evaluate their safety and security: “Where do you feel most comfortable and safe?”
- Action-focused thinking: “If you could change your environment to help you better meet your goals, how would you do so?”
What to do next…
Look at the big picture.
By now you understand how seemingly unrelated factors, like someone’s relationships and work life, might affect their ability to lose fat, gain muscle, and/or improve their overall health.
So for the best results, assess every client for Deep Health—even if they have a super-specific aesthetic goal.
Dig for connections.
The social bone is connected to the mental bone, is connected to the physical bone, and so on. Pull a thread of your client’s life with curiosity, assuming that things are related, and see what it unravels.
This also means that small specific things are a microcosm. If a client comes to you with big problems, ask for particular, concrete examples of how those problems manifested. For instance:
Client: I eat terribly.
Coach: Can you tell me a specific situation in the last day or two where you ate terribly? Like one meal, maybe? What was happening then?
And so on.
Collaborate with your client.
Don’t tell, direct, lecture, or immediately jump in with “helpful” suggestions.
Instead: Investigate, together. Ask, learn, listen.
Every client needs a unique approach, and they need to buy in, first. That happens when they feel autonomous and self-determined, and when they get to tell their story without judgment from the coach.
All you have to do to create an individualized plan is to ask the right questions, and listen to the answers.
Remember that coaching is a science, but it’s also an art.
The science of nutrition can get your clients abs. Artful coaching can make their lives better. Combine the two, and you’re setting yourself (and your clients) up for success.
If you’re a coach, or you want to be…
You can help people build sustainable nutrition and lifestyle habits that will significantly improve their physical and mental health—while you make a great living doing what you love. We’ll show you how.
If you’d like to learn more, consider the PN Level 1 Nutrition Coaching Certification. (You can enroll now at a big discount.)
The post Level 1: The “Deep Health” coaching secret that transforms short-term fitness goals into life-changing results appeared first on Precision Nutrition.
Do you want to lose weight? Gain muscle? Improve health? Boost performance? This free calorie, portion, and macro calculator from Precision Nutrition can help you achieve the results you want… more easily than ever before.
Ready to try it? Click “Get Started” below and enter your information to instantly calculate calories, portions, and macros.
(Once we calculate your macros, we’ll send you a free, personalized guide to using our hand portion system for hitting your calorie and macro targets.)
![]()

© Precision Nutrition
What makes this macro calculator so great?
Designed, developed, and tested in the Precision Nutrition research lab—and proven effective with thousands of clients—it’s the most comprehensive calorie, portion, and macro calculator available.
Here’s why: The Precision Nutrition Calculator first determines the appropriate daily calories for your body, based on the NIH Body Weight Planner (and adapted from research collected at the National Institute of Diabetes and Digestive and Kidney Disease).
This estimate takes into account:
- Your personal details (height, age, weight, sex)
- Physical activity levels (both daily movement and purposeful exercise)
- The date you want to reach your goal by (within reason!)
- The changing and adaptive nature of human metabolism (a major benefit of this calorie calculator)
It then calculates your daily macros, combining the above data with additional factors, including your:
- Nutrition and fitness goals (weight loss, muscle gain, body recomposition, better health, peak performance)
- Dietary preference (Paleo, keto, vegetarian, fully plant-based, Mediterranean, and of course, “anything”)
- Macronutrient preference (balanced, low-fat, low-carb, or virtually any other macronutrient ratio you want)
But here’s the reason this calorie calculator is truly revolutionary: Once it estimates your calorie and macronutrient needs, it automatically converts those numbers into food portions that are equivalent to parts of your hand. (Specifically, your palm, fist, cupped hand, and thumb.)
The result: If you choose, you can skip weighing and measuring your food—as well as logging the details of every meal into calorie and macro tracking apps. Instead, you can use our hand portion tracking system to achieve your calorie and macro targets.
This unique approach takes the hassle out of calorie and macro tracking, making it easier for you to lose weight, gain muscle, eat healthier, and improve your performance.
The benefits of this calorie, portion, and macro calculator
Some people naturally eat the appropriate amount of food and calories for their individual needs. They’re able to maintain a stable body weight for years—even decades— without counting how many calories they eat, or tracking macros, or ever measuring their portions.
Unfortunately, these “intuitive eaters” represent only a small segment of the human population. The rest of us typically need help with our eating, in the form of external structure and guidance, at least temporarily. This can help you:
- Eat the right number of calories and macros for your goals
- Understand appropriate portion sizes
- Improve your food choices and eating habits
That’s why we created this calorie, portion, and macro calculator. It gives you a nutrition blueprint for achieving your goals and, at the same time, helps you develop the skills you need to eat well for life.
(For optimal results, it’s best to combine this nutrition plan with intuitive eating and self-regulation skills.)
The problem with only tracking calories
Most people know calories matter. If you eat more calories than your body needs, you gain weight. If you eat fewer calories than your body needs, you lose weight.
(Yes, this certainly sounds simple, but as you’ve likely experienced, there are many factors that make managing your calorie intake… not so simple. Learn more here.)
By tracking how many calories you eat, you can better know if you’re consuming the right amount of food for your goals. There are, however, disadvantages to only tracking the total number of calories you eat daily.
Most notably: This method doesn’t ensure you’re getting an appropriate amount of macronutrients for your body, goals, and preferences. Depending on what you’re trying to achieve, this can negatively affect your appetite, hormones, energy levels (especially for physical activity), and nutrient consumption.
And that can make it harder to lose weight, gain muscle, eat healthier, and improve athletic performance.
Why tracking your macros gives you an advantage
Just in case you’re not sure, let’s start by defining what macros, or macronutrients, actually are.
There are three major macronutrients: Protein, carbohydrates, and fat. (The fourth macronutrient is alcohol.)
Your body breaks down the macronutrients you eat into compounds used to help create energy, build body structures, create chemical reactions, and stimulate the release of hormones. Which means they can impact how you feel, perform, and even behave.
When you track macros, you don’t need to count calorie intake directly. Instead, you log how many grams of each macronutrient you eat every day.
That’s because each macronutrient provides a certain number of calories:
- 1 gram of protein = 4 calories
- 1 gram of carbohydrate = 4 calories
- 1 gram of fat = 9 calories
- (1 gram of alcohol = 7 calories)
As a result, tracking macros means you’re automatically tracking calorie intake. It’s just that you’re ensuring a certain number of calories come from protein, carbohydrates, and fat, respectively. This is known as your macronutrient ratio.
For example, let’s say you eat:
- 30% of your calories from protein
- 40% of your calories from carbohydrate
- 30% of your calories from fat
Your macronutrient ratio would then be: 30:40:30.
By adjusting your macronutrient ratio based on your age, sex, activity levels, goals, and preferences, you can optimize your eating plan.
If you’re trying to lose weight, you might eat a higher proportion of protein, since it can help you feel satisfied longer after meals. Or if you’re a very physically active athlete, you might want a higher ratio of carbohydrates to meet your greater energy demands.
The good news: Our calorie, portion, and macro calculator will figure all of this out for you.
Just enter your information and, within milliseconds, you’ll get a macro ratio that’s customized exactly for your body, goals, and preferences. (Plus, the Precision Nutrition Calculator gives you the option to further adjust these numbers, in case you want to try a different macronutrient ratio.)
Like calorie counting, though, conventional macro tracking has its downsides. Perhaps the biggest challenge: Because it requires careful food measuring and weighing, most people won’t stick to it for long.
Many say it feels cumbersome and even takes the joy out of eating. Which can limit its effectiveness to very short periods of time. That’s where the Precision Nutrition hand portion tracking system comes in.
Hand portions: The easiest way to track calories and macros
When we created this calorie, macro, and portion calculator, we asked:
How can we help people eat the right amount of food, but without the burden of having to weigh and measure every morsel?
Our solution: to give personalized targets not just for daily calories and macros, but also hand portions. That way, you can use whichever method you prefer.
This hand portion system—developed by Precision Nutrition—allows you to use your own hand as a personalized, portable portioning tool. You’re not actually measuring your food, but rather using your hand to gauge portion size. It’s highly effective for food tracking because your hand is proportionate to your body, its size never changes, and it’s always with you.
Here’s a snapshot of how it works:
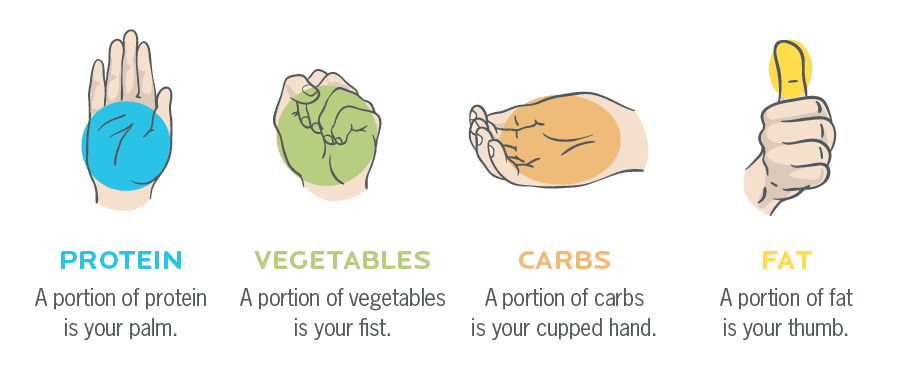
- Your palm determines your protein portions.
- Your fist determines your vegetable portions.
- Your cupped hand determines your carb portions.
- Your thumb determines your fat portions.
Based on the calorie, portion, and macro calculator’s output, all you have to do is eat the recommended number of each hand portion daily. (Again, we’ll show you how to put this method fully into practice once you’ve put your information into the Precision Nutrition Calculator and received your free report and eating guide.)
How effective are hand portions for tracking macros?
Our research shows hand portions are 95 percent as accurate (or better) as carefully weighing, measuring, and tracking. With substantially less effort and time involved.
Plus, our hand portion tracking system allows you to easily adjust your intake to further optimize your results.
Ready to get started? Go ahead and enter your information into the calorie, portion, and macro calculator above, and we’ll do the rest, providing you with a free nutrition plan customized just for you.
If you have more questions right now, or want to understand the nutrition rules we used to design this calorie, portion, and macro calculator, see the Resources section for a full breakdown.
If you’re a coach, or you want to be…
You can help people build sustainable nutrition and lifestyle habits that will significantly improve their physical and mental health—while you make a great living doing what you love. We’ll show you how.
If you’d like to learn more, consider the PN Level 1 Nutrition Coaching Certification. (You can enroll now at a big discount.)
The post The Ultimate Calorie, Portion, and Macro Calculator appeared first on Precision Nutrition.
15 Jul, 2021 | Admin | No Comments
How to count (and track) macros for fat loss, muscle gain, and better health
What are macros? | How to calculate your macros | How to track your macros | Macros troubleshooting and FAQs | What to eat on a macro diet | How to measure portions | Macros and consistency | Macros for weight loss | Macros and alcohol
Lose weight, gain muscle, and perform better.
But in exchange, you have to do math.
Still with us?
Then maybe you’d like to learn how to count macros.
Counting macros is a way to track food intake using grams of protein, carbs, and fats (macronutrients) instead of calories.
The advantage of focusing on macronutrients over calories is that it tells you a bit more about the quality of your food, and how it affects your body.
The disadvantage of tracking macros is that you have to plan, measure, and record everything you eat. And then you have to do math to add up your macronutrient tallies at the end of each day.
For most people, that can be a bit confusing and intimidating, especially when you first get started.
That’s why we created this comprehensive guide to everything macros.
You’ll learn:
- What macronutrients are and what foods contain them
- How to calculate and track your personal macronutrients
- Why macronutrients aren’t the full story when it comes to health
- Who macronutrient tracking works best for (and who it doesn’t)
Let’s go.
.pncta-l1-banner {
width: 90%;
max-width: 90%;
min-height: 262px;
padding: 0;
display: block;
margin: 1rem auto 3rem;
box-shadow: rgba(0,0,0,.08) 0 0 6px 0;
box-sizing: border-box;
background: #2b363e radial-gradient(circle at 78% 56%,#435360,#2b363e 53%);
overflow: hidden;
height: auto;
}
.pncta-l1-shape {
position: relative;
width: 65%;
height: 70px;
margin: -40px auto 30px auto;
background: #068FB9;
text-align: center;
border-radius: 15%/50%;
padding-top: 45px;
box-sizing: border-box;
}
.pncta-l1-shape:after {
content: “”;
position: absolute;
top: -95%;
bottom: -15%;
right: -5%;
left: -5%;
background: inherit;
border-radius: 15%/50%;
}
.pncta-l1-over {
position: relative;
z-index: 200;
color: #fff;
padding: 0;
margin: 0 auto;
font-size: 14.5px;
font-weight: 200;
text-align: center;
width: 100%;
}
.pncta-l1-over > strong {
font-size: 23px
}
.pncta-l1-row:after {
content: “”;
display: table;
clear: both
}
.pncta-l1-content {
position: relative;
display: flex;
margin: 15px 27px;
flex-direction: row;
align-items: normal;
overflow: hidden;
background: url(https://www.precisionnutrition.com/wp-content/uploads/2020/07/img-book-ipad.png) no-repeat;
height: 100%;
width: auto;
background-size: contain;
background-position: 100% 0;
min-height: 180px;
}
.pncta-l1-content-launch {
position: relative;
margin: 15px 27px;
align-items: normal;
overflow: hidden;
height: 100%;
width: auto;
min-height: 180px;
}
.pncta-l1-info {
padding: 0;
margin: 0;
text-align: left;
width: 60%;
overflow: hidden;
}
.pncta-l1-info-launch {
padding: 0;
margin: 0;
text-align: left;
width: 100%;
overflow: hidden;
}
.pncta-l1-info h3, .pncta-l1-info-launch h3 {
font-size: 23.5px;
font-weight: 700;
font-stretch: normal;
font-style: normal;
line-height: normal;
letter-spacing: normal;
color: #fff!important;
padding: 0 0 10px;
}
.pncta-l1-info p, .pncta-l1-info-launch p {
text-align: left;
padding: 0 0 15px 0;
margin: 0;
font-size: 14.5px;
font-stretch: normal;
font-style: normal;
line-height: 1.37;
letter-spacing: normal;
color: #c6cbce;
font-weight: 400;
width: 90%;
}
.pncta-l1-img {
width: 40%;
position: relative
}
.pncta-l1-img > img {
display: none;
margin: 0;
position: absolute;
top: 1em;
right: 0;
left: 0;
max-width: 100%;
margin: 0 auto;
z-index: 2;
}
.pncta-l1-btn {
color: #f4f4f4 !important;
width: 180px;
height: 34px;
text-transform: uppercase;
font-size: 13.5px;
font-weight: 600;
font-stretch: normal;
font-style: normal;
line-height: normal;
letter-spacing: normal;
text-align: center;
min-width: 180px;
background: linear-gradient(to bottom,#068FB9 2%,rgba(41,151,186,.96)),linear-gradient(to bottom,#1fd8ff,rgba(31,216,255,0) 6%);
line-height: 0;
border-radius: 2.4px!important
}
a.pncta-l1-addbanner:active, a.pncta-l1-addbanner:hover, a.pncta-l1-addbanner:link, a.pncta-l1-addbanner:visited {
color: none !important;
text-decoration: none!important;
outline: 0!important
}
@media only screen and (max-width: 768px) {
.pncta-l1-banner {
min-height: 232px;
}
.pncta-l1-over {
font-size: 13px;
}
.pncta-l1-over > strong {
font-size: 21px;
}
.pncta-l1-content {
min-height: auto;
margin: 15px 27px 25px;
}
.pncta-l1-content-launch {
min-height: auto;
margin: 15px 27px 25px;
}
.pncta-l1-info h3, .pncta-l1-info-launch h3 {
font-size: 21px
}
}
@media only screen and (max-width: 767px) {
.pncta-l1-btn {
font-size: 14px;
}
.pncta-l1-shape {
width: 75%
}
.pncta-l1-banner {
min-height: 232px
}
.pncta-l1-over {
font-size: 13px;
}
.pncta-l1-over > strong {
font-size: 17px
}
.pncta-l1-content {
min-height: auto;
background-size: 44%;
margin: 15px 35px
}
.pncta-l1-content-launch {
min-height: auto;
background-size: 44%;
margin: 15px 35px
}
.pncta-l1-info h3, .pncta-l1-info-launch h3 {
font-size: 17px
}
.pncta-l1-info p, .pncta-l1-info-launch p {
font-size: 13px;
}
}
@media only screen and (max-width: 580px) {
.pncta-l1-shape {
width: 80%
}
.pncta-l1-banner {
min-height: 232px
}
.pncta-l1-over {
font-size: 13px
}
.pncta-l1-over > strong {
font-size: 17px;
}
.pncta-l1-content {
min-height: auto;
background-size: 50%;
margin: 15px
}
.pncta-l1-content-launch {
min-height: auto;
background-size: 50%;
margin: 15px
}
.pncta-l1-info h3, .pncta-l1-info-launch h3 {
font-size: 14px
}
.pncta-l1-info p, .pncta-l1-info-launch p {
font-size: 13px
}
}
@media only screen and (max-width: 500px) and (orientation: portrait) {
.pncta-l1-content {
background: 0 0;
}
.pncta-l1-banner {
width: 100%;
margin: 1rem auto;
min-height: 380px;
max-width: 100%
}
.pncta-l1-shape {
position: relative;
width: 75%;
height: 80px}
.pncta-l1-info p,.pncta-l1-over{font-size: 13px;
display: table}.pncta-l1-info h3,.pncta-l1-over>strong{font-size: 17px;
line-height: initial!important;
font-weight: 600;
}
.pncta-l1-content {
flex-direction: column;
align-items: baseline;
margin: 0 auto;
text-align: center;
padding: 0 15px;
width: 100%;
height: 320px;
background-size: 50%;
background-position: bottom center}
.pncta-l1-content-launch {
flex-direction: column;
align-items: baseline;
margin: 0 auto;
text-align: center;
padding: 0 15px;
width: 100%;
height: 320px;
background-size: 50%;
background-position: bottom center}
.pncta-l1-img,.pncta-l1-info,.pncta-l1-info p,.pncta-l1-info>h3,.pncta-l1-info-launch,.pncta-l1-info-launch p,.pncta-l1-info-launch>h3{width: 100%;
display: block;
text-align: center;
margin: 0 auto}.pncta-l1-img>img{display: block}.pncta-l1-content: after{content: “”;
display: inline-block;
width: 0;
height: 0;
border-style: solid;
border-width: 0 100px 50px 100px;
border-color: transparent transparent #068FB9 transparent;
z-index: 0;
transform: scale(3.5);
left: 0;
right: 0;
position: absolute;
bottom: 0;
margin: 0 auto;
text-align: center
}
}
Save $200 on the industry’s top nutrition certification
Help people improve their health and fitness—while making a great full-time or part-time living doing what you love.
–>
What are macros, anyway?
Macros, or macronutrients, are large groups of nutrients.
There are three main macronutrients: Protein, carbohydrates, and fat.
(Technically, alcohol is a fourth macronutrient, but nutrition plans don’t focus on it because it doesn’t offer much in terms of health benefits.)
Most foods and beverages are made up of a combination of these three macronutrients. But many foods have one dominant macronutrient that provides the majority of the calories.
For example:
- Brown rice is mostly carbohydrate but also has a bit of protein and fat.
- Cashews are mostly fat but also contain protein and a bit of carb.
- Lean chicken breast is mostly protein but also contains some fat. It doesn’t contain any carbohydrates.
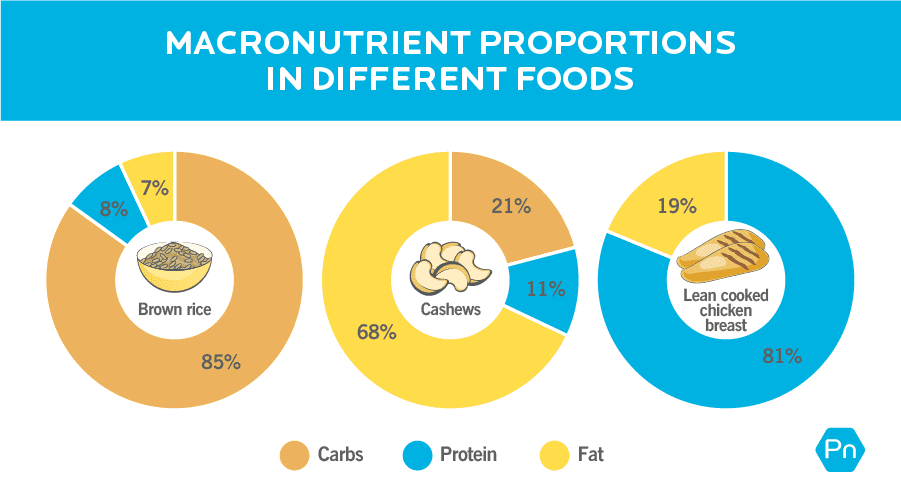
Each macronutrient provides a certain number of calories:
- 1 gram of protein = 4 calories
- 1 gram of carbohydrate = 4 calories
- 1 gram of fat = 9 calories
- (1 gram of alcohol = 7 calories)
As a result, tracking macros means you’re automatically tracking calories.
Why are macronutrients important?
Your body breaks down macronutrients to perform specific jobs in the body.
For example:
- Proteins break down into amino acids, which can affect our muscle composition, and are involved in creating mood-regulating neurotransmitters.
- Carbohydrates break down into sugars, which give us energy for immediate use, but also storage.
- Fats break down into fatty acids, which help form certain structures of our body, like our brain, nervous system, and cell walls.
So, in addition to impacting your body weight and composition, macronutrients can impact how you feel, perform, and even behave.
How to calculate your macros
If you’re eager to get your personalized macros plan, a heads up before you start:
Once you get your macro numbers, you’ll want to stick to them for at least two weeks.
It takes that long to determine whether any changes you notice are due to your plan working (or not working), or just regular body fluctuations.
After two weeks, you can evaluate how things are going, and adjust your calories / macros up or down as needed. All of the methods below provide estimates of your daily calorie and macro needs, so in most cases, it takes some experimenting before you find what works for you.
Ok, let’s crunch those numbers.
Step 1: Calculate your energy (calorie) needs.
Macro counting is based on the calories in, calories out (CICO) principle: When you take in more energy than you burn, you gain weight, and when you take in less energy than you burn, you lose weight.
(Learn why CICO is indisputable: Calories in vs. out? Or hormones? The debate is finally over.)
So before you work out your macros, you have to figure out your energy (calorie) requirements, based on your body, lifestyle, and goals.
Here are two ways to do that.
Option 1: Use our Macros Calculator.
There are plenty of nutrition calculators out there, but ours is—lowkey brag coming up—special.
Most calculators determine your maintenance calorie needs using static formulas. Then, they simply chop 500 calories per day or lower the calories 10 to 20 percent below maintenance—no matter how much weight someone wants to lose or in what time frame.
Our Macros Calculator does two things that are unique:
- It factors in the date you want to achieve your goal by. For example, the time you plan to take to gain muscle or lose weight.
- It accounts for metabolic adaptation. As you lose weight, you burn fewer calories. As you gain weight, you burn more calories. In other words, your body tries to compensate for weight loss by slowing your metabolism a bit, and for weight gain by speeding up your metabolism a bit. Other calculators don’t consider this.
![]()
© Precision Nutrition
To use it, plug in your personal details and goals, and you’ll get your estimated daily calorie needs.
If you use our calculator, you can just skip Step 2 below. Because along with your calorie estimates, you’ll also get recommendations for your ideal macronutrient ratio—or the option to customize it yourself.
Option 2: Use the chart below.
For people who love by-hand calculations, we’ve got you.
First, find your activity level and goal below.
Then, multiply your bodyweight in pounds by the corresponding multiplier.
Daily calorie estimator
| Client goal | |||
| Lose weight | Maintain weight | Gain weight | |
| Lightly active (<3 hrs / wk) |
10-12 | 12-14 | 16-18 |
| Moderately active (3-7 hrs / wk) |
12-14 | 14-16 | 18-20 |
| Very active (<7 hrs / wk)* |
14-16 | 16-18 | 20-22 |
* Competitive athletes—who are often active for over 15 hours per week—have even higher needs.
For example, a lightly active 170-pound person who wants to lose weight would eat between 1,700 and 2,040 calories each day.
Women should generally start at the lower end of the range, and men at the higher end. Or, start in the middle and see what happens. If you’re not seeing the desired results, adjust calorie intake up or down accordingly.
Note: These short-hand multipliers become less accurate as you move away from “average” body weights. For individuals who are very light, very large, or very muscular, our macros calculator above might be more accurate.
Step 2: Determine your macronutrient ratio.
Your macronutrient ratio (also called your “macronutrient split”) refers to how much of each macronutrient you’re eating.
For most people, a good split is 15 to 35 percent protein, 40 to 60 percent carbohydrates, and 20 to 40 percent fat.
(This is just a framework. You can modify these proportions according to your preferences. And if you follow a high fat or high carb diet, your numbers may go outside these ranges.)
By adjusting your macro ratio based on your age, sex, activity levels, goals, and preferences, you can personalize your eating plan for your optimal health.
Use our Macros Calculator as mentioned above, or the formulas below.
We’ll cover each macronutrient one at a time.
Protein
Your protein needs will depend on your weight, activity level, and goals.
We calculate protein first because it’s essential for so many aspects of good health, including fat loss, muscle gain and maintenance, and athletic performance and recovery.
Use the charts below to figure out how much protein you need in grams per pound or kilogram of bodyweight.
| PROTEIN NEEDS IN G/LB | |||
| Maintenance / improve health | Fat loss / body recomposition | Muscle gain | |
| Lightly active (<3 hours/week) |
0.6 to 0.9 | 0.7 to 1.0 | 0.8 to 1.1 |
| Moderately active (3-7 hours/week) |
0.7 to 1.0 | 0.8 to 1.1 | 0.9 to 1.2 |
| Highly active (>7 hours/week) |
0.8 to 1.1 | 0.9 to 1.2 | 1.0 to 1.3 |
| PROTEIN NEEDS IN G/KG | |||
| Maintenance / improve health | Fat loss / body recomposition | Muscle gain | |
| Lightly active (<3 hours/week) |
1.3 to 2.0 | 1.5 to 2.2 | 1.8 to 2.4 |
| Moderately active (3-7 hours/week) |
1.5 to 2.2 | 1.8 to 2.4 | 2.0 to 2.6 |
| Highly active (>7 hours/week) |
1.8 to 2.4 | 2.0 to 2.6 | 2.2 to 2.9 |
If you’re new to healthy eating or have a hard time getting protein into your diet, start with the lower end of the range.
If you’re ready for more advanced nutrition protocols, or you’re a dedicated exerciser, aim for the higher end.
So, a 170-pound nutrition beginner who’s lightly active and wants to lose fat might choose the factor 0.8 g/lb from the range 0.7 to 1.0.
170 pounds x 0.8 = 136 grams of protein / day
A highly active 165-pound experienced lifter who wants to gain muscle might choose the factor 1.2 g/lb from the range 1.0 to 1.3.
165 pounds x 1.2 = 198 grams of protein / day
Note: For professional athletes, lean individuals trying to get very lean, and experienced lifters trying to minimize fat gain when adding body weight, protein requirements may go as high as 1.5 g/lb or 3.3 g/kg.
Fat & Carbohydrates
How much you eat of these two macros depends on, well, what you like.
First, figure out how many calories and what percentage of your macros you have left over after protein.
The formula looks like this (recall each gram of protein has four calories):
Total calories – (Total grams of protein x 4 calories) = Fat and carb calories
To get your protein percentage, divide calories from protein by total calories:
Calories from protein / Total calories = Percent of total calories from protein
Now, subtract your percent of protein from 100 to get your percent of fat and carbohydrates. (Home stretch, folks!)
100 – Percent of calories from protein = Percent of fat and carbs
Then you can decide how you want to split fat and carbs.
Here are some factors to consider:
- In general, the more active you are, the greater your carbohydrate needs.
- The minimum threshold for fat is 15 to 20 percent of total calories.
- Research shows that low-fat and low-carb diets work equally as well for weight loss.1
Let’s say, after a person subtracts their percent of calories from protein, they have 75 percent of calories left over to use on either fat or carbs. And they decide to do 50 percent carbs (4 calories per gram) and 25 percent fat (9 calories per gram).
Here’s how to do the math:
Carbohydrates:
Total calories x 0.5 = Carbohydrate calories
Carbohydrate calories / 4 = Grams of carbohydrates
Fat:
Total calories x 0.25 = Fat calories
Fat calories / 9 = Grams of fat
Keto macros: How low carb can you go?
The ketogenic diet was originally developed to treat epilepsy. Physicians discovered that fasting reduced the frequency of seizures, but so did an extremely low-carb diet.
Eventually, bodybuilders and fitness enthusiasts got wind of the diet and thought, ‘If the ketogenic diet mimics fasting, maybe I can get ripped without having to drop calories too low and lose all my gainz.’
A couple of decades later, everyone is eating cauliflower-crust keto pizza. (It’s actually pretty good.)
In terms of the macros split, the ketogenic diet consists of about 70-90 percent calories from fat, with the remaining 10-30 percent of calories coming from a mix of carbohydrates and protein combined.
(For comparison, a standard “low carb” diet is about 50 percent fat, 30 percent protein, and 20 percent carbohydrate.)
Unless you’re trying to stay in ketosis for medical reasons (to reduce seizures), less strict versions of the keto diet—which allow higher amounts of protein and carbs—are more sustainable for most people, especially athletes trying to maintain performance and muscle mass.
(Interested in trying—or coaching—the ketogenic diet? Here’s your primer: The Keto diet plan: Your complete how-to guide.)
How to track your macros
Once you’ve determined your macros, you’ll want to track them to ensure that you’re meeting your macronutrient goals each day.
Most people use an app like MyFitnessPal, Cronometer, or Macros+.
There are a couple of advantages to using an app:
- You have a quick reference guide for how much of each macronutrient a serving of a food contains
- The app will add up your macros for you (and let you know how many you have left for the day)
Or, you can keep track of your macros by hand, using a paper journal and a nutrition database like the USDA’s Food Data Central or SELFNutritionData.
With either approach, record the foods you’ve eaten at each meal, along with how many grams of each macronutrient each food contains.
Many people find it helps to plan meals the night before or the morning of. This helps you strategize ahead of time, building meals that meet your macro goals, instead of choosing food reactively when you’re starving and—oh man, that giant burrito looks good.
Most apps also allow you to save meals. So if you tend to repeat meals every once and awhile, having pre-entered and -calculated food combinations can make tracking more efficient.
If you plan on dining out, logging ahead of time can be a good strategy for sticking to your macros. Check out the menu before you get to the restaurant, and do your best to estimate the macros of the meal you’ll order.
5 common questions about macro tracking
Once you’ve figured out your macro numbers, you might feel like you have the key to all your future health and fitness goals.
Until you actually have to eat.
“Wait…how do I do this in real life?!”
Here are some of the most common questions people have about tracking macros, and what to do.
Question 1: What do you eat on a macro diet?
As you get used to tracking your macros, you’ll learn which foods are high in protein, carbs, and fat.
But one thing macronutrient counting doesn’t take into account is micronutrients (vitamins and minerals, usually found in whole, minimally processed foods).
Micronutrients are necessary for good health. And though you probably could hit your macros by crushing pizza, french fries, and protein shakes, we wouldn’t suggest it.
As a macro counter, it’s up to you to ensure you eat a diet that meets your macro- and micronutrient needs.
One simple way to do that?
Hit your macros primarily through a variety of minimally processed foods that are naturally rich in micronutrients: lean proteins, fruits and vegetables, whole grains and legumes, nuts and seeds, and pressed oils.
If you’re not sure where to start, check out the graphic below. You can see that while some foods fit neatly into certain macronutrient categories, other foods are more of a mix.
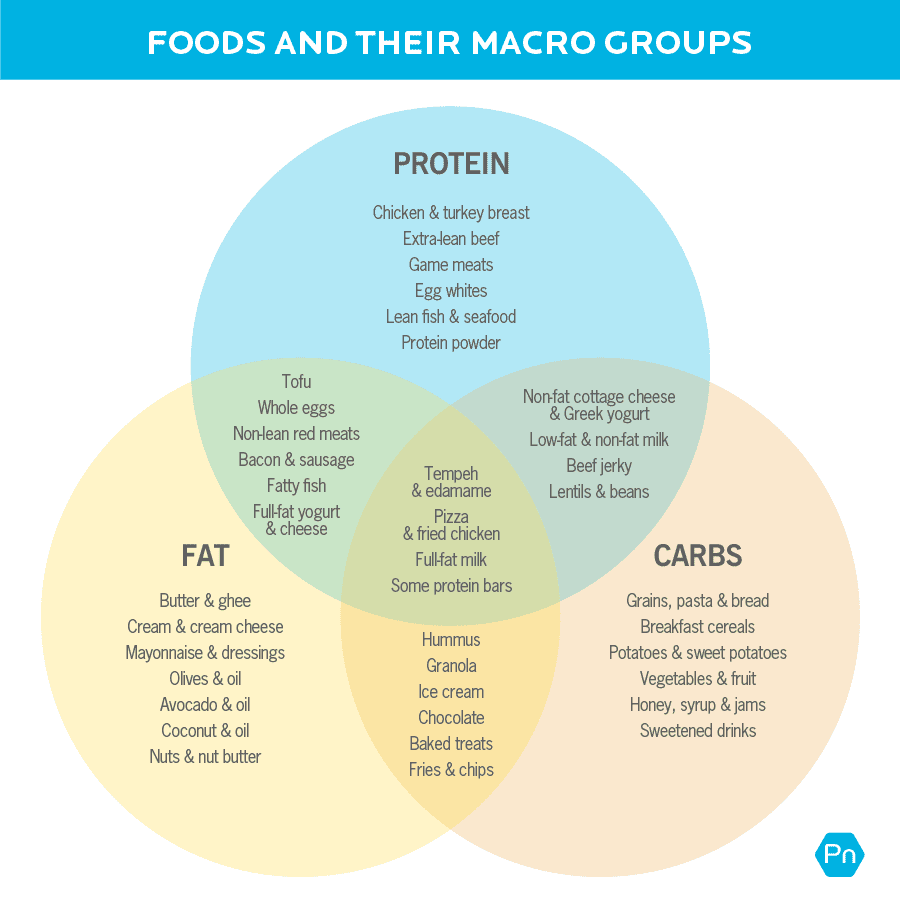
(For a more detailed version of the above image, check out our handout: The Macros Chart.)
Question 2: How do I measure my food?
It’s not quite Sophie’s choice, but people still wonder:
Should I measure food by volume (with a measuring cup) or by weight (with a food scale)?
Use a food scale for the best results. Measuring by weight will always be more accurate than measuring by volume.
For example, depending on whether they’re whole or chopped, a cup will fit about 100 grams of almonds. But if those almonds are finely chopped, they’re easier to pack in, and a cup may fit 200 grams.
On a scale, 100 grams will always be a 100 grams, no matter if the almonds are whole or chopped.
But if your only option is measuring cups and spoons, that’s ok. Just be sure—especially in the beginning—to measure everything, rather than eyeball it.
People tend to overestimate what a “tablespoon” or “cup” looks like, sometimes unintentionally doubling their portion.
Note: Cooking certain foods like grains, pasta, and meat, can change their weight and volume. So, if you measure a food raw, log it raw. If you measure it cooked, log it cooked.
If weighing and measuring your food feels tedious and soul-shrivelling, there are other tracking options.
For example, you could track your intake using hand portions. Our Macros Calculator provides hand portions too, so you don’t have to meticulously measure everything (unless you want to).
(Learn all about hand portions here: How your fist, palm, cupped hand, and thumb can help you avoid the hassle of counting calories.)
Question 3: How important is it to precisely hit my macros?
Consistency will get you the results you want.
But that doesn’t mean you have to hit your macros exactly every single day.
If you’re having a bad week (or year) remember that 50 percent consistency is better than giving up completely.
(Need proof that you don’t need to be perfect to get results? Read: One million data points show what it REALLY takes to change your body.)
If you feel like you’re really flailing, just prioritize meeting your protein goals each day. A diet higher in protein will help reduce hunger, preserve muscle, and help improve overall health.
Overall, aim for consistency over perfection. Try to get close to your daily macro goals, but don’t force yourself to eat if you’re not hungry.
And if you’d rather have half an avocado than a bowl of oatmeal? Don’t stress about swapping fat for carbs.
Question 4: Can you use macros for weight loss?
If your goal is to lose fat, it’s a good idea to use some kind of method to track food intake, at least for a period of time.
Many people use calories. But macros account for calories, and have the added value of telling you a bit more about food quality (like the amount of protein, fat, or carbohydrate in a food).
Especially for weight loss—where the goal is usually to lose fat but maintain lean mass—tracking macros can help ensure you get enough muscle-preserving protein while still eating fewer calories than you burn.
Use the protein recommendations chart above to find the protein range for your goal and activity level. If your goal is to lose fat, minimize hunger, and preserve muscle mass, choose the upper end of your range.
From there, figure out your carb and fat allowances, remembering that to lose fat, you have to eat fewer calories than you burn—also called a calorie deficit—for a period of time.
Question 5: How do I track alcohol?
Just because alcohol isn’t included in typical macro plans doesn’t mean you can’t have it.
But you should track it, since it contains calories.
The most common way to do this is to use some of your fat or carbohydrate grams to account for the alcohol.
For instance, if you’re having a beer, 12 ounces is approximately 155 calories.2
If you want to exchange it for carbohydrates, do the following equation:
155 calories / 4 calories per gram = 38.75 grams
So you could log your lager as 39 grams of carbs.
Or if you’re having a glass of red wine, a 5-ounce serving is 127 calories.3
To use fat grams for that glass:
127 calories / 9 calories per gram = 14.1 grams
So you could log your vino as 14 grams of fat.
Or, just use a combination of carbs and fat, by dividing the calories however you see fit and repeating the steps above.
What to do next
Ready to get started? Here are some things to keep in mind before you begin.
Know what you hope to accomplish.
Macro counting works well for people with specific goals.
As you progress towards or even achieve your goal, consider if you want to continue counting macros. Some people enjoy counting them indefinitely, but most eventually get tired of tracking.
Truth is, macro counting is just one of many nutrition strategies you can add to your toolbox.
(Want another awesome strategy? Read: The 30-day eating challenge that can blow your mind—and transform your body.)
Treat macro counting as an experiment.
The first macro split you try might work great. Or not.
Whether you succeed or fail, don’t use it as a proxy for your self-worth.
Gather your data, and just see what happens. Stay open-minded, and use the outcome of your experiment to inform your next choices.
Did you enjoy tracking macros, and feel closer to your goals? Cool! Keep going.
Did all the measuring and counting feel too finicky and left you stressed out? Try a different way of improving your nutrition.
(And if you REALLY loved working with macros, you might like our continuing education course: How to Coach a Macros-Based Diet.)
It’s okay if macro counting isn’t for you.
Full disclosure: At Precision Nutrition, macronutrient counting isn’t our go-to method of regulating food intake. At least, not for most people.
Macro counting works—especially for high-level, advanced goals, like preparing for a physique competition or a major athletic event.
But despite the fact that macro counting can be super flexible, it’s also a lot of work. Especially compared to other methods of “watching what you eat,” which can be just as effective.
For most people and most goals, there are less labor-intensive ways to get results. Here are some ideas:
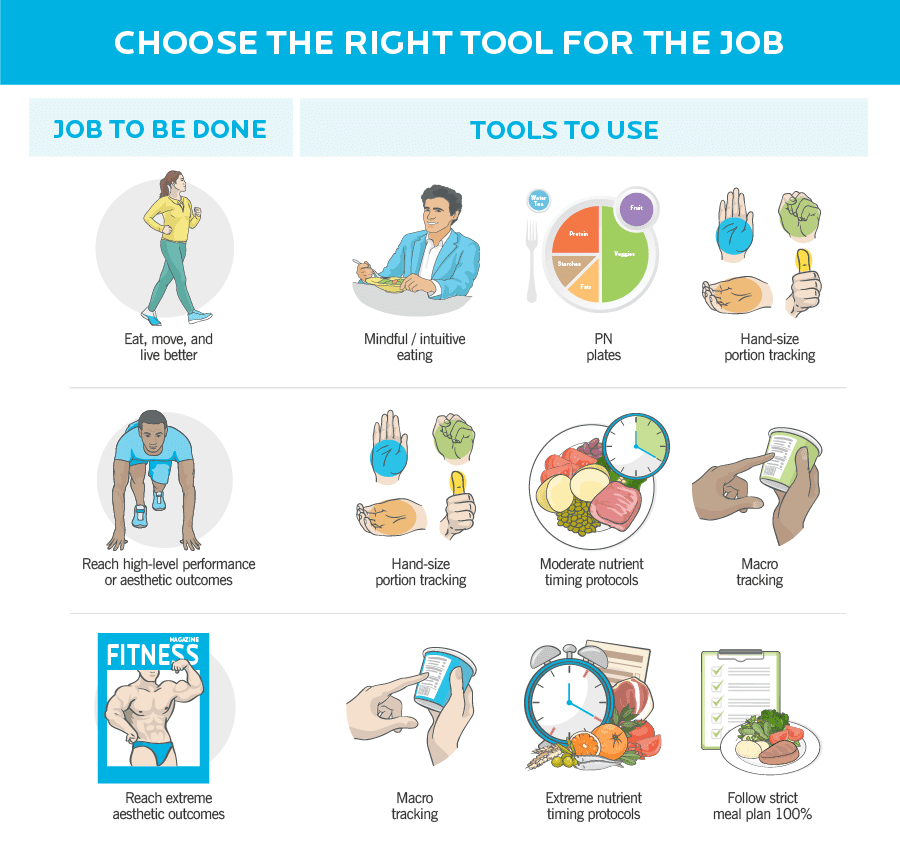 (Want to compare different methods of food tracking? Read: Macros vs. calories vs. portions vs. intuitive eating.)
(Want to compare different methods of food tracking? Read: Macros vs. calories vs. portions vs. intuitive eating.)
Remember that we eat food, not nutrients.
Food is so much more than grams of protein, carbohydrates, and fat. And meals aren’t just a chance to hit your macro goals.
Meals are also an opportunity to experience pleasure, spend time caring for your body, and share with people you love.
Every meal is a chance to connect—with yourself and with others. And every food choice is an opportunity to direct, shape, and remake your health.
jQuery(document).ready(function(){
jQuery(“#references_link”).click(function(){
jQuery(“#references_holder”).show();
jQuery(“#references_link”).parent().hide();
});
});
References
Click here to view the information sources referenced in this article.
1. Sacks, Frank M., George A. Bray, Vincent J. Carey, Steven R. Smith, Donna H. Ryan, Stephen D. Anton, Katherine McManus, et al. 2009. “Comparison of Weight-Loss Diets with Different Compositions of Fat, Protein, and Carbohydrates.” The New England Journal of Medicine 360 (9): 859–73.
2. “FoodData Central.” n.d. Accessed July 15, 2021. https://fdc.nal.usda.gov/fdc-app.html#/food-details/344427/nutrients.
3. “FoodData Central.” n.d. Accessed July 15, 2021. https://fdc.nal.usda.gov/fdc-app.html#/food-details/173190/nutrients.
If you’re a coach, or you want to be…
You can help people build sustainable nutrition and lifestyle habits that will significantly improve their physical and mental health—while you make a great living doing what you love. We’ll show you how.
If you’d like to learn more, consider the PN Level 1 Nutrition Coaching Certification. (You can enroll now at a big discount.)
The post How to count (and track) macros for fat loss, muscle gain, and better health appeared first on Precision Nutrition.
22 Apr, 2021 | Admin | No Comments
Keep showing up: 5 people who met their body transformation goals during the COVID-19 crisis.
When these clients joined Precision Nutrition Coaching in January of 2020 to improve their health and lives, the plan was straightforward: Follow the program and trust the process.
Two months in, the COVID-19 pandemic hit. Nothing in life was straightforward.
Overnight, many were facing food shortages, financial instability, and overwhelming uncertainty.
It would have been understandable for these five people to press pause on their health and fitness efforts.
But they didn’t.
Instead, they listened to the little voice in their heads that said: ‘keep going.’
Every person highlighted in this article faced challenges in the past year: medical issues, forced business closure, heightened anxiety, the loss of a loved one… The list goes on.
Despite these obstacles, they kept showing up for themselves—chipping away at their goals, a little bit at a time.
Over the course of 12 months, they achieved incredible physical transformations.
Even more impressive? The unexpected ways these five people changed their lives, and the powerful lessons they took from their experiences.
++++
Victor: In the midst of grief, he lost 25 pounds and found a new purpose in life.
In his early forties, Victor Salgado, now 47, developed diabetes. He managed this condition with three to four injections of insulin every day. He also took eight other medications to treat additional health concerns, including high blood pressure.
That was Victor’s life for nearly five years.
In 2018, desperate for change, he signed up for coaching with a PN-Certified Coach. In that year, he lost nearly 50 pounds and, on the advice of his doctors, he stopped taking insulin injections and blood pressure medication.
“For the last two years, I haven’t taken one single prescription medication—not a shot,” he says proudly.
Victor’s experience working with a coach made him realize he wanted to help others too, so he became a personal trainer and earned his Precision Nutrition Level 1 Certification. (And in the fall of 2020, he graduated from the Precision Nutrition Level 2 program!)
However, it wasn’t all smooth sailing from there. Towards the end of 2019, Victor was struggling again.
“I’m a veteran suffering from PTSD. For a while, I wasn’t doing enough to keep myself busy. And when that happens, your mind goes to other places.”
Victor knew he needed something to focus on, a place to direct his energy. He thought back to his experience working with a coach, and signed up for Precision Nutrition Coaching.
Right before he joined, Victor, newly married, moved from South Carolina to California to be with his extended family. “Adjusting to a new family life in a new place was very challenging.”
In addition to adapting to a new, well, everything, Victor soon faced another challenge: The pandemic.
The gym where Victor had just begun to find comfort and community shut down.
He tried to adapt his gym workouts to at-home ones, but affordable equipment was hard to come by. So he took up running.
Even when temperatures rose to unbearable levels (think: 130℉), Victor found a way to make it work. “I woke up at 3:30am to be outside by 4am. Even then it would already be 97℉.”
At one point, his neighbors asked if he was getting tired of running every day. His answer?
“I got tired of taking insulin three to four times a day, pricking my finger three to four times a day. That got me tired. But running? No.”
Eventually, he built some workout equipment out of metal bars and concrete. (He calls it his “Fred Flinstone” gym.) Every now and then, his 11-year-old daughter will ask to train with him, which makes him smile.
Toward the end of the year, Victor and his wife contracted COVID-19. “My heart rate became really high. My doctor suggested I dial back my workouts, so I eased up. But I didn’t stop. Eventually, my heart rate went back to normal.”
Victor’s mother-in-law, who lived with him, also contracted the virus. She passed away shortly after, in December of 2020.
“That was one of the most challenging things I’ve had to endure in quite some time. I’m pretty sure that if I hadn’t developed a mindset of resilience with the help of PN, I would’ve been paralyzed.”
After making it through one of the most difficult periods of his life, Victor decided to do something to pay it forward.
“I’ve been working on establishing a coaching business. Yesterday, I began training my first online client.”
Silvia: A scary diagnosis made her believe she’d never run again. But she regained her strength and defied the odds.

In her early thirties, Silvia Pontuschka was diagnosed with osteoarthritis in both of her hips.
“It felt like I was being handed a life sentence of misery,” she remembers.
By her mid-thirties, the pain had become so severe that she found it difficult to walk. She would wake up in the middle of the night stiff and in agony.
“I was afraid of my future,” she recalls. “Was this something I just had to live with forever? Would I have to have a hip replacement in my forties? I felt so limited in terms of what I was allowed to do. The pain felt like a reminder that life would never be ‘normal.’”
Silvia knew she couldn’t just wait around to see what would happen. She had to take action.
Silvia had previously signed up for Precision Nutrition Coaching, but didn’t make it through the whole year due to the stress of an international move.
This time around, she felt ready to fully commit, but she knew she’d need as much support as possible. After Silvia chatted with her sister about her plans, her sister volunteered to do a weekly check-in for added moral support.
“That sealed the deal for me. It was the push I needed to sign up,” she says.
Silvia quickly found her groove. She maintained much closer contact with her PN coach this time around. She also trained at her gym three times a week, and over the course of a few short months, she felt her body getting stronger.
But soon, COVID-19 meant her gym had to close.
Silvia tried to make the best of the situation. She decided to turn her living room into a makeshift gym, and took advantage of the program’s minimal equipment workout routines.
This worked for Silvia at the start. But eventually, she felt something was missing when she trained alone.
So, she found another accountability partner—a workout buddy.
Soon, Silvia’s daily workouts became the anchor of her day, helping her to stick to a routine when everything else seemed turned upside down.
After weeks, then months, Silvia noticed her body becoming stronger.
“Four modified push-ups before needing a break became seven, then ten, which then became sets of full push-ups.”
And the debilitating pain in her hips?
It was still an issue halfway through the year, so she decided to employ a strategy from her PN Coaching lessons: She kept things simple.
Silvia added one glute-focused exercise to her routine. And as she felt able, she gradually added more targeted exercises to support her hip mobility.
“Showing up continually and slowly increasing my strength, mobility, and the length of my daily walks for the last six months of the program resulted in better flexibility, less pain, and the ability to do something I thought was no longer possible: go for runs!”
Silvia even began to look for more ways to move her body. She took daily afternoon walks, opted to use her condo stairs instead of the elevator, and sought out hills on her bike rides.
“The more I moved, the more I realized my body is designed to do exactly that. Every movement became a way to honor my body and admire how marvelous it is.”
The best part: “This was all achieved not by being perfect and doing grand gestures, but by just showing up and doing what I could do with the time, energy, and resources I had in the moment.”
Bradley: He regained control of his health after a decade of pain—and lost 80 pounds.

A decade ago, Bradley was in a car accident, which broke his back in four places, leaving him with ongoing pain.
A few years later, he developed sciatica-like pain due to arthritis, which made exercise almost unbearable. Not long after, he developed rashes, which his doctor treated with a steroid regimen.
And with that treatment came unwanted weight gain.
The extra weight aggravated his previous back injury and further limited his ability to work out.
“I was completely broken, physically and mentally. I was hopeless.”
As Bradley reached a low point, he connected with someone who’d recently finished Precision Nutrition Coaching. They told him the program could help, and Bradley was game to try anything—so he signed up.
“When I started out, I couldn’t do any of the exercises without severe pain. I had to take it very easy,” he remembers. Bradley focused on stretching daily, taking walks on his treadmill, and practicing the program’s eating habits.
Within a few weeks, he began to notice weight loss.
Then the pandemic hit. Yet another roadblock. Bradley could hardly believe it.
As a healthcare lab technician, Bradley was thrown into a grueling schedule performing COVID-19 tests. Like many other frontline workers, the demands of his job left him with little energy for his own health.
Every day provided another legitimate reason for Bradley to break the momentum he was building with nutrition and fitness. But he kept leaning on a big, undeniable reason to keep going:
“I had to get myself better. Not just for me, but for my family.”
So he did what he could, when he could, and worked on “just a little bit better” each day. He continued to lose weight.
The more Bradley lost, the better he felt. After nearly a decade of feeling stuck, the ball was rolling.
Bradley felt like he was finally getting his health back on track.
“Losing weight was almost easy after a while, because I wasn’t focused on losing weight, but on healing,” Bradley says.
By the end of the year, Bradley had lost 80 pounds and 53 total inches. And with the reduced strain on his body, his pain levels went from debilitating pangs to mild, occasional aches.
Now, he’s finally back to his favorite hobby: bowling in leagues and tournaments.
His biggest takeaway?
“Completing the program during the pandemic made me realize that I can make time for my health, no matter the circumstances.”
Lindsey: When her business shut down, she found solace in nutrition and fitness, losing 14 pounds in the process.

At 34 years old, Lindsey Marvin’s weight, insomnia, and anxiety were at an all-time high.
Money was tight at the taproom and restaurant Lindsey owns with her husband. The business is a labor of love for the couple, so she was working 14-hour days back-to-back to keep it afloat.
That mean Lindsey’s health and wellness fell to the bottom of her to-do list. “I was stress-eating the first thing I saw just so I could get back to work. I felt totally out of control,” she says.
One day, Lindsey realized some of her favorite clothes weren’t fitting anymore.
And the idea of putting on a swimsuit? No way.
That marked a turning point. “Going to the beach is my absolute favorite thing, so I knew I needed to make some changes.”
The previous year, Lindsey saw her husband lose 60 pounds with the help of Precision Nutrition Coaching. “He was more confident and in control than I had ever seen,” she says. So she decided to sign up too.
Nearly halfway through the coaching year, a curveball: Her restaurant was mandated to shut down due to COVID-19.
“Seeing the restaurant emptied out was very emotional for me,” Lindsey says. “Starting and growing a small business is like having a baby. The thought of it failing is traumatic.”
But that empty space that initially felt so uncomfortable to be in?
Lindsey got creative and turned the empty taproom into her own personal gym.
She used bags of sugar as weights. She filled kegs to varying levels and used those too.
“After I started working out in my makeshift workout space, I started to regain some feeling of control over the situation,” she recalls.
Despite all the uncertainties she faced, this was a place where she could let it all go and focus on doing something for herself.
“Moving my body every day and planning my meals made everything else feel doable. I learned to control what I could and stop stressing about the things I couldn’t.”
Lindsey was making progress not just physically, but mentally too.
Working with her doctor, Lindsey slowly weaned off the medication she’d been taking for anxiety and insomnia. At the same time, she picked up some new coping strategies.
“I started knitting before bed instead of watching TV or scrolling through my phone. It was just enough mental stimulation to keep me from boredom, and it occupied my hands so I didn’t want to snack late at night.”

When gyms were allowed to reopen their doors, Lindsey took one of the Precision Nutrition Coaching lessons to heart: She stepped out of her comfort zone and tried something new.
She joined a (real) gym and hired a personal trainer.
“I had reservations about having a trainer. But having Coach Gillian support me made me feel more open to trying it. I absolutely love being coached now.”
By the end of 2020, Lindsey lost 16 total inches and gained a new approach to looking after her health:
“When I started PN, I was obsessed with the number on a scale. I thought I needed to spend hours weighing food, and always be perfect. Now I know it’s about an accumulation of small things that add up to something bigger. I don’t need to go all out on anything. I just need to think about myself, what I want, and be a little bit better every day.”
Philip: At 61, he got his health and fitness back on course with small, simple shifts in the right direction.

When Philip Davis started Precision Nutrition Coaching, he was on a “gentle, but nonetheless apparent, downward slide.”
While he’d always done a fair amount of walking, Philip’s friends pointed out that he would choose the least hilly route on their walks. He also noticed he was winded climbing the steep hill to his home.
Philip knew his physical fitness was in decline.
And the health markers he was keeping track of—blood pressure, cholesterol, body fat percentage, and weight—were all going up.
“I was starting to not like how I looked in the mirror. My clothes weren’t fitting as well. And on one occasion, a pal even commented on my ‘dad bod’!”
Philip knew he didn’t want physical decline to become his new normal.
But he debated what to do next: Stay on the same course? Or start moving more and eating differently?
Philip knew his huffing-and-puffing up the hill was related to what he calls poor eating choices: too much wine at dinner and a tendency to frequent neighborhood bakeries.
So when he joined the program, he was eager to improve his diet. But knew it would be a process, and that his efforts could backfire if he felt deprived.
He understood that he wouldn’t be able to completely change his habits overnight. But what he discovered was that he didn’t have to. (Check out PN’s body transformation research to find out why.)
Philip told himself that if he “just kept showing up,” he would be able to adopt new habits—healthier habits—that would stick.
The way Philip sees it, forming new habits is like sailing a boat. If you change a boat’s direction by a few degrees, this slight adjustment can dramatically alter its final destination.
Throughout the year, Philip experienced occasional “lapses.” Instead of being discouraged by these setbacks, he focused on how he could improve a little bit each day.
And the steep hill to his house? Philip barely notices it now.
He enjoys his daily walks up his neighborhood’s steep hills.
In fact, Philip and his wife now seek out hills on their daily walks:
“There’s one particular walk we take in the mornings that includes a 500-foot elevation gain in half a mile. That’s when I feel all those squats from the PN exercise program proving their worth!”
Twelve months later, Philip is 15 pounds leaner and quite a bit stronger.
“I have a more proactive outlook on my health and fitness that will serve me well today, tomorrow, and for the rest of my life.”
Want help becoming the healthiest, fittest, strongest version of you?
Most people know that regular movement, eating well, sleep, and stress management are important for looking and feeling better. Yet they need help applying that knowledge in the context of their busy, sometimes stressful lives.
Over the past the past two decades, we’ve used the Precision Nutrition Coaching method to help over 150,000 clients lose fat, get stronger, and improve their physical and mental health… for the long-term… no matter what challenges they’re dealing with.
It’s also why we work with health, fitness, and wellness professionals (through our Level 1 and Level 2 Certification programs) to teach them how to coach their own clients through the same challenges.
<!–
Interested in Precision Nutrition Coaching? Join the presale list now. You’ll get a free gift today, save up to [pnc_discount], and have the chance to secure a spot 1 week early.
We’ll be opening up spots in our next Precision Nutrition Coaching on [launch_date program=”pnc” type=”general” dateformat=”l, F jS, Y”].
If you’re interested in coaching and want to find out more, join the presale list below. Being on the list gives you three special advantages.
- You’ll pay less than everyone else. Join the presale list and you’ll save up to [pnc_discount] off the general public price.
- You’re more likely to get a spot. To give clients the personal care and attention they deserve, we only open up the program twice a year. By joining the presale list you’ll get the opportunity to register a week before everyone else, increasing your chances of getting in.
- You’ll get a free gift—plus an inside look at the program. When you join the presale list today, we’ll send you a free 35-page ebook: Your Best Nutrition Starts Here—a complete guide to building a health plan for your body, goals, and lifestyle (no calorie-counting or restrictive dieting required). Plus, you’ll get our new Enrollment Packet, giving you an inside look at the PN Coaching program, complete with stories from past clients who’ve overcome huge obstacles and achieved the transformation of their dreams, and more.
If you’re ready to change your body, and your life, with help from the world’s best coaches, this is your chance.
[Note: If your health and fitness are already sorted out, but you’re interested in helping others, check out our Precision Nutrition Level 1 Certification program].
–>
The post Keep showing up: 5 people who met their body transformation goals during the COVID-19 crisis. appeared first on Precision Nutrition.